NIVEL (Netherlands Institute for Health Services Research), PB 1568, 3500, BN, Utrecht, the Netherlands.
BMC Palliat Care. 2012 Sep 18;11:17. doi: 10.1186/1472-684X-11-17.
Our aim was to obtain a clearer picture of the relevant care experiences and care perceptions of incurably ill Turkish and Moroccan patients, their relatives and professional care providers, as well as of communication and decision-making patterns at the end of life. The ultimate objective is to improve palliative care for Turkish and Moroccan immigrants in the Netherlands, by taking account of socio-cultural factors in the guidelines for palliative care.
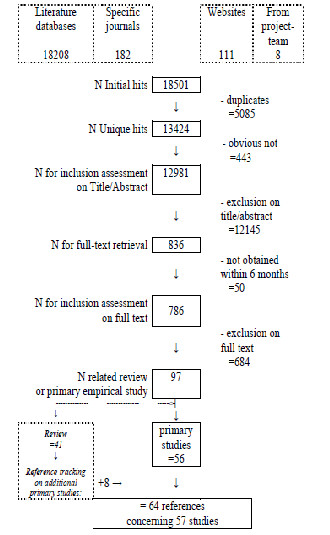
A systematic literature review was undertaken. The data sources were seventeen national and international literature databases, four Dutch journals dedicated to palliative care and 37 websites of relevant national and international organizations. All the references found were checked to see whether they met the structured inclusion criteria. Inclusion was limited to publications dealing with primary empirical research on the relationship between socio-cultural factors and the health or care situation of Turkish or Moroccan patients with an oncological or incurable disease. The selection was made by first reading the titles and abstracts and subsequently the full texts. The process of deciding which studies to include was carried out by two reviewers independently. A generic appraisal instrument was applied to assess the methodological quality.
Fifty-seven studies were found that reported findings for the countries of origin (mainly Turkey) and the immigrant host countries (mainly the Netherlands). The central themes were experiences and perceptions of family care, professional care, end-of-life care and communication. Family care is considered a duty, even when such care becomes a severe burden for the main female family caregiver in particular. Professional hospital care is preferred by many of the patients and relatives because they are looking for a cure and security. End-of-life care is strongly influenced by the continuing hope for recovery. Relatives are often quite influential in end-of-life decisions, such as the decision to withdraw or withhold treatments. The diagnosis, prognosis and end-of-life decisions are seldom discussed with the patient, and communication about pain and mental problems is often limited. Language barriers and the dominance of the family may exacerbate communication problems.
This review confirms the view that family members of patients with a Turkish or Moroccan background have a central role in care, communication and decision making at the end of life. This, in combination with their continuing hope for the patient's recovery may inhibit open communication between patients, relatives and professionals as partners in palliative care. This implies that organizations and professionals involved in palliative care should take patients' socio-cultural characteristics into account and incorporate cultural sensitivity into care standards and care practices.
我们的目的是更清楚地了解绝症土耳其和摩洛哥患者及其亲属和专业护理提供者的相关护理经验和护理感知,以及生命终末期的沟通和决策模式。最终目标是通过在姑息治疗指南中考虑社会文化因素,改善荷兰土耳其和摩洛哥移民的姑息治疗。
进行了系统的文献回顾。数据源包括 17 个国家和国际文献数据库、4 种专门从事姑息治疗的荷兰期刊以及 37 个相关国家和国际组织的网站。检查了所有找到的参考文献,以确定它们是否符合结构化的纳入标准。纳入仅限于处理社会文化因素与患有肿瘤或绝症的土耳其或摩洛哥患者的健康或护理状况之间关系的初级实证研究的出版物。选择是通过首先阅读标题和摘要,然后再阅读全文来进行的。两位审查员独立决定纳入哪些研究。应用通用评估工具评估方法学质量。
发现了 57 项研究,这些研究报告了原籍国(主要是土耳其)和移民东道国(主要是荷兰)的研究结果。核心主题是家庭护理、专业护理、临终关怀和沟通的经验和看法。家庭护理被视为一种责任,即使这种护理对主要女性家庭照顾者来说尤其成为严重负担。许多患者和亲属更喜欢专业的医院护理,因为他们在寻求治疗和安全。临终关怀深受恢复希望的强烈影响。亲属在临终决策中经常具有相当大的影响力,例如决定停止或停止治疗。很少与患者讨论诊断、预后和临终决策,并且关于疼痛和心理问题的沟通往往有限。语言障碍和家庭的主导地位可能会加剧沟通问题。
本综述证实了这样一种观点,即具有土耳其或摩洛哥背景的患者的家庭成员在生命终末期的护理、沟通和决策中起着核心作用。这一点,再加上他们对患者康复的持续希望,可能会抑制患者、亲属和专业人员作为姑息治疗伙伴之间的开放沟通。这意味着参与姑息治疗的组织和专业人员应考虑患者的社会文化特征,并将文化敏感性纳入护理标准和护理实践。