Agenzia Provinciale per la Protonterapia, Via F.lli Perini, 181, 38122, Trento, Italy.
Radiat Oncol. 2012 Sep 18;7:160. doi: 10.1186/1748-717X-7-160.
To validate, in the context of adaptive radiotherapy, three commercial software solutions for atlas-based segmentation.
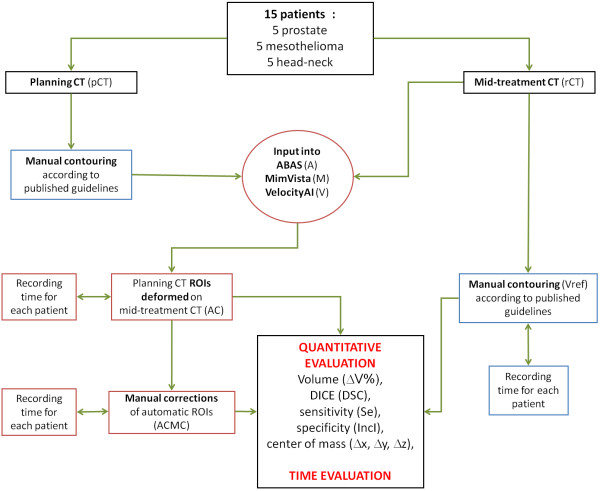
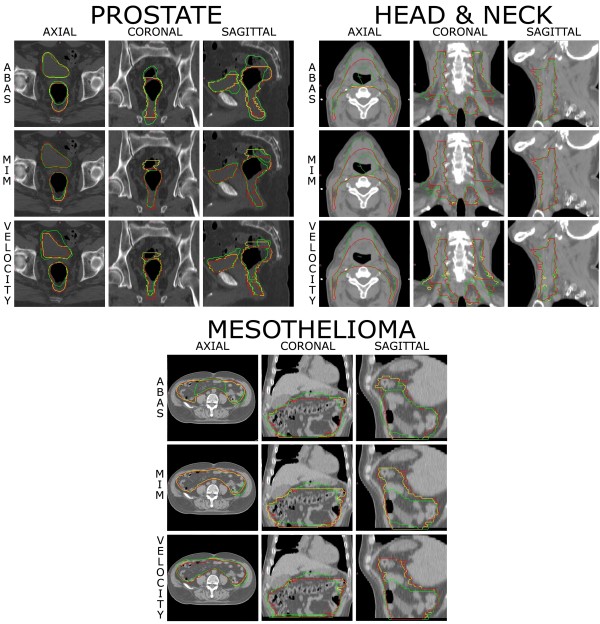
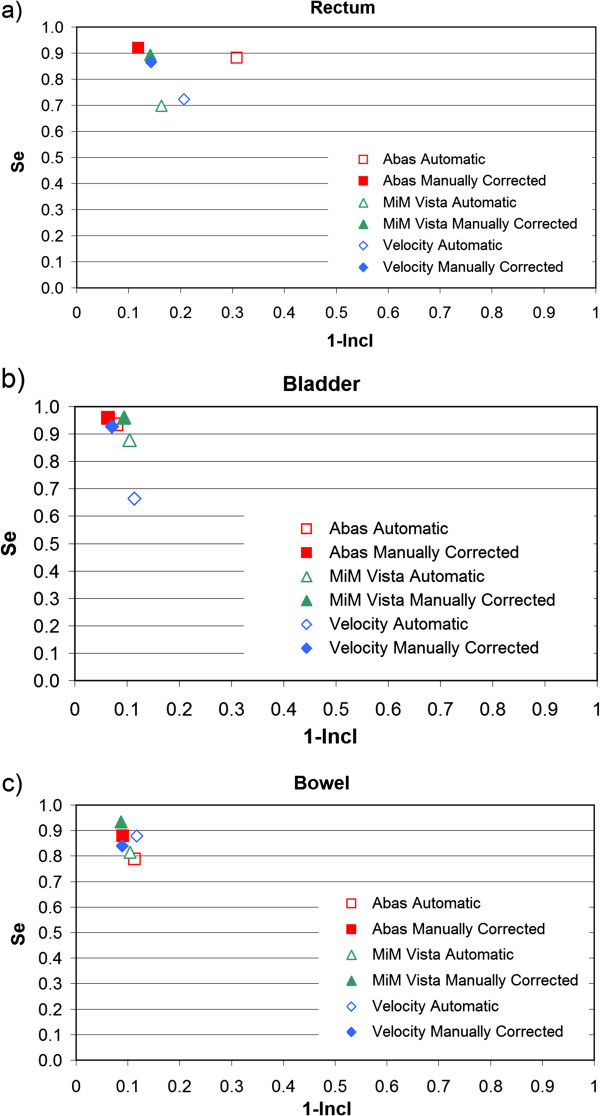
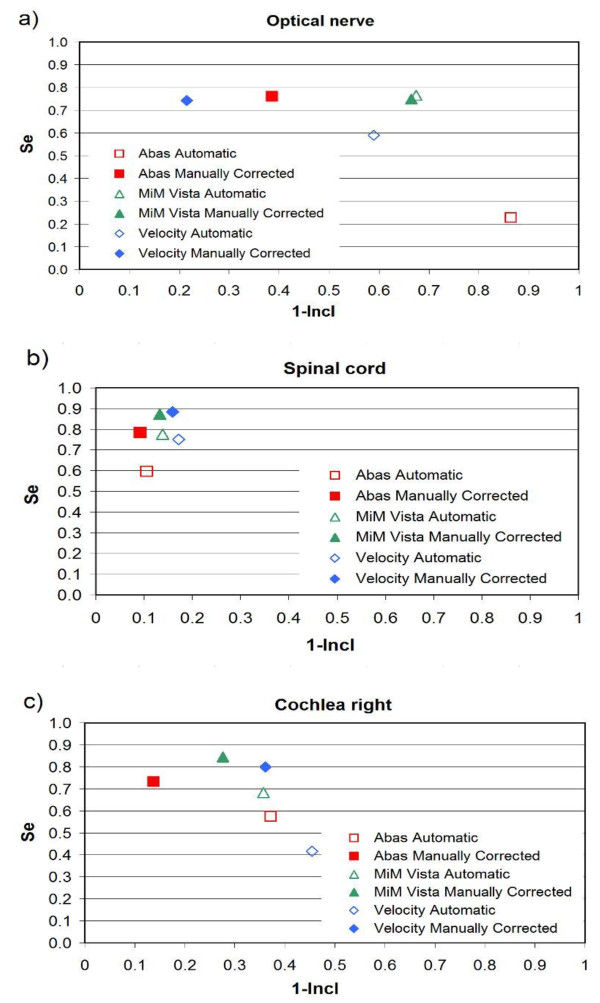
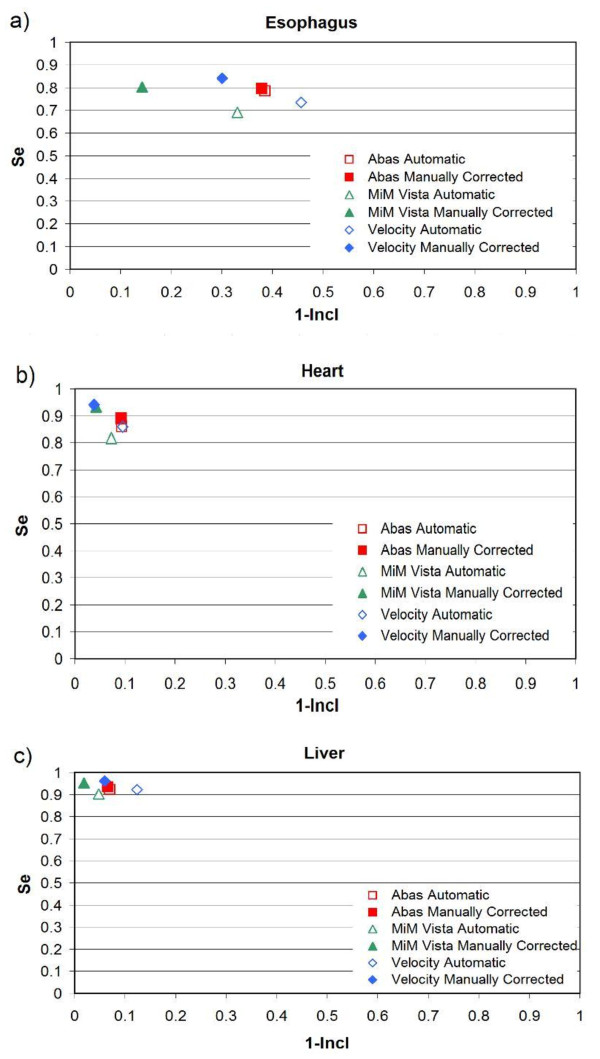
Fifteen patients, five for each group, with cancer of the Head&Neck, pleura, and prostate were enrolled in the study. In addition to the treatment planning CT (pCT) images, one replanning CT (rCT) image set was acquired for each patient during the RT course. Three experienced physicians outlined on the pCT and rCT all the volumes of interest (VOIs). We used three software solutions (VelocityAI 2.6.2 (V), MIM 5.1.1 (M) by MIMVista and ABAS 2.0 (A) by CMS-Elekta) to generate the automatic contouring on the repeated CT. All the VOIs obtained with automatic contouring (AC) were successively corrected manually. We recorded the time needed for: 1) ex novo ROIs definition on rCT; 2) generation of AC by the three software solutions; 3) manual correction of AC.To compare the quality of the volumes obtained automatically by the software and manually corrected with those drawn from scratch on rCT, we used the following indexes: overlap coefficient (DICE), sensitivity, inclusiveness index, difference in volume, and displacement differences on three axes (x, y, z) from the isocenter.
The time saved by the three software solutions for all the sites, compared to the manual contouring from scratch, is statistically significant and similar for all the three software solutions. The time saved for each site are as follows: about an hour for Head&Neck, about 40 minutes for prostate, and about 20 minutes for mesothelioma. The best DICE similarity coefficient index was obtained with the manual correction for: A (contours for prostate), A and M (contours for H&N), and M (contours for mesothelioma).
From a clinical point of view, the automated contouring workflow was shown to be significantly shorter than the manual contouring process, even though manual correction of the VOIs is always needed.
在自适应放疗的背景下,验证三种基于图谱的分割商业软件解决方案的有效性。
本研究纳入了 15 名癌症患者,每组 5 名,包括头颈部、胸膜和前列腺癌患者。除了治疗计划 CT(pCT)图像外,每位患者在放射治疗过程中还获得了一套重新计划 CT(rCT)图像。三位经验丰富的医生在 pCT 和 rCT 上勾画了所有感兴趣的体积(VOI)。我们使用三种软件解决方案(VelocityAI 2.6.2(V)、MIMVista 5.1.1(M)的 MIM 和 CMS-Elekta 的 ABAS 2.0(A))在重复 CT 上生成自动勾画。所有通过自动勾画(AC)获得的 VOI 都依次手动校正。我们记录了以下三个方面的时间:1)rCT 上重新定义 ROI;2)三种软件解决方案生成 AC;3)AC 的手动校正。为了比较软件自动生成的体积与 rCT 上从头勾画的体积的质量,我们使用了以下指标:重叠系数(DICE)、敏感性、包含指数、体积差异和三个坐标轴(x、y、z)上的位移差异。
与从头手动勾画相比,三种软件解决方案在所有部位上节省的时间均具有统计学意义,且三种软件解决方案的节省时间相似。每个部位的节省时间如下:头颈部约 1 小时,前列腺约 40 分钟,间皮瘤约 20 分钟。对于前列腺,A(轮廓)、A 和 M(H&N 轮廓)以及 M(间皮瘤轮廓)获得了最佳的 DICE 相似系数指数。
从临床角度来看,自动勾画工作流程明显短于手动勾画过程,尽管总是需要对 VOI 进行手动校正。