Department of Postgraduate General Practice Education, NHS Education for Scotland, 2 Central Quay, Glasgow, Scotland G3 8BW, United Kingdom.
BMC Health Serv Res. 2012 Oct 8;12:351. doi: 10.1186/1472-6963-12-351.
A significant minority of patients do not receive all the evidence-based care recommended for their conditions. Health care quality may be improved by reducing this observed variation. Composite measures offer a different patient-centred perspective on quality and are utilized in acute hospitals via the 'care bundle' concept as indicators of the reliability of specific (evidence-based) care delivery tasks and improved outcomes. A care bundle consists of a number of time-specific interventions that should be delivered to every patient every time. We aimed to apply the care bundle concept to selected QOF data to measure the quality of evidence-based care provision.
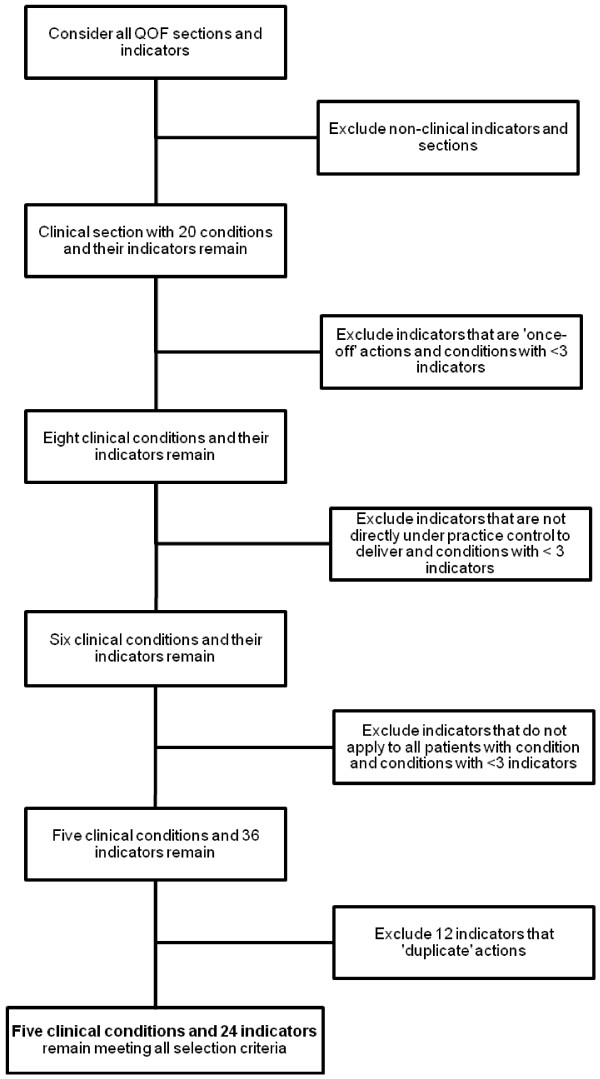
Care bundles and components were selected from QOF indicators according to defined criteria. Five clinical conditions were suitable for care bundles: Secondary Prevention of Coronary Heart Disease (CHD), Stroke & Transient Ischaemic Attack (TIA), Chronic Kidney Disease (CKD), Chronic Obstructive Pulmonary Disease (COPD) and Diabetes Mellitus (DM). Each bundle has 3-8 components. A retrospective audit was undertaken in a convenience sample of nine general medical practices in the West of Scotland. Collected data included delivery (or not) of individual bundle components to all patients included on specific disease registers. Practice level and overall compliance with bundles and components were calculated in SPSS and expressed as a percentage.
Nine practices (64.3%) with a combined patient population of 56,948 were able to provide data in the format requested. Overall compliance with developed QOF-based care bundles (composite measures) was as follows: CHD 64.0%, range 35.0-71.9%; Stroke/TIA 74.1%, range 51.6-82.8%; CKD 69.0%, range 64.0-81.4%; and COPD 82.0%, range 47.9-95.8%; and DM 58.4%, range 50.3-65.2%.
In this small study compliance with individual QOF-based care bundle components was high, but overall ('all or nothing') compliance was substantially lower. Care bundles may provide a more informed measure of care quality than existing methods. However, the acceptability, feasibility and potential impact on clinical outcomes are unknown.
少数患者未接受其病情所需的所有循证护理。通过减少这种观察到的差异,医疗质量可能会得到提高。综合措施为质量提供了一种不同的以患者为中心的视角,并通过“护理捆绑包”概念在急症医院中用作特定(基于证据)护理提供任务和改善结果的可靠性指标。护理捆绑包由许多特定时间的干预措施组成,应每次为每位患者提供。我们旨在将护理捆绑包概念应用于选定的 QOF 数据,以衡量基于证据的护理提供质量。
根据定义的标准,从 QOF 指标中选择护理捆绑包和组件。五种临床情况适合护理捆绑包:冠心病(CHD)、中风和短暂性脑缺血发作(TIA)、慢性肾脏病(CKD)、慢性阻塞性肺疾病(COPD)和糖尿病(DM)的二级预防。每个捆绑包有 3-8 个组件。在苏格兰西部的九家普通医疗实践中进行了回顾性审计。收集的数据包括向特定疾病登记册中包含的所有患者提供个别捆绑包组件的情况(或未提供)。使用 SPSS 计算实践水平和捆绑包及组件的整体合规性,并以百分比表示。
九家实践(64.3%),患者总数为 56948 人,能够按照要求提供数据格式。根据开发的基于 QOF 的护理捆绑包(综合措施),总体合规性如下:CHD 为 64.0%,范围为 35.0-71.9%;中风/TIA 为 74.1%,范围为 51.6-82.8%;CKD 为 69.0%,范围为 64.0-81.4%;COPD 为 82.0%,范围为 47.9-95.8%;DM 为 58.4%,范围为 50.3-65.2%。
在这项小型研究中,个别基于 QOF 的护理捆绑包组件的合规性很高,但总体(“全部或无”)合规性要低得多。护理捆绑包可能为护理质量提供比现有方法更明智的衡量标准。然而,其可接受性、可行性和对临床结果的潜在影响尚不清楚。