Epidemiology Postgraduate Program, Federal University of Pelotas, Pelotas, Brazil.
J Adolesc Health. 2012 Dec;51(6 Suppl):S38-45. doi: 10.1016/j.jadohealth.2012.08.016. Epub 2012 Nov 10.
To investigate the effect of obesity at the start of adolescence on the prevalence, incidence and maintenance of chest wheezing among individuals aged 11-15 years in a birth cohort in a developing country.
The seventh follow-up of the 1993 Pelotas birth cohort occurred in 2004 (individuals aged 10-11 years). Between January and August 2008, the eighth follow-up of the cohort was conducted. All the individuals of the original cohort who were alive (who were then adolescents aged between 14 and 15 years) were targets for the study. The International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire was used to define wheezing. In addition to the body mass index (BMI), used to define obesity by the World Health Organization (WHO) criteria, we assessed skinfold thickness.
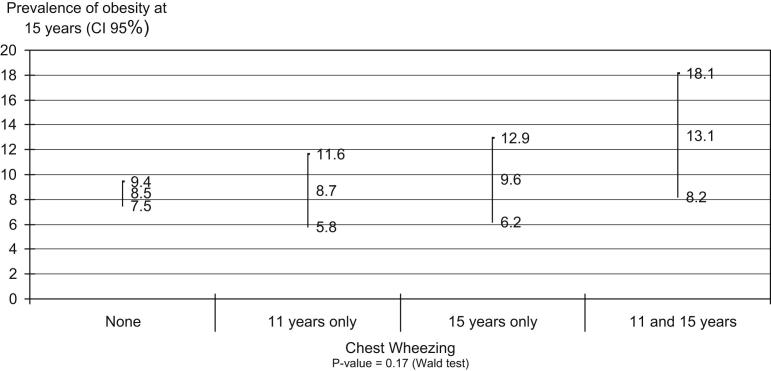
From the original cohort, 4,349 individuals were located (85.7% follow-up rate). The prevalence of chest wheezing at 11 and 15 years were 13.5% (95% CI: 12.5%-14.5%) and 12.1% (95% CI: 11.1%-13.1%), respectively. The prevalence of wheezing at both times was 4.5% (95% CI: 3.9%-5.1%) and the incidence of wheezing was 7.5% (95% CI: 6.7%-8.3%). Independent of the effect of various confounding variables, the prevalence of wheezing at 15 years was 50% greater among obese individuals than among eutrophic individuals at 11 years (RR 1.53; 95% CI: 1.14-2.05). The greater the skinfold tertile at 11 years, the higher the prevalence of wheezing at 15 years was (p = .011). Weight status and skinfolds did not present any association with incident wheezing. After controlling for confounding factors, the risk of persistent wheezing among obese individuals at 11 years was 1.82 (95% CI: 1.30-2.54).
Since obesity at the start of adolescence is associated with asthma symptom persistence, prevention and treatment of obesity may reduce avoidable healthcare costs and disease burden.
研究青春期起始时肥胖对发展中国家青少年人群(11-15 岁)中胸部喘息患病率、发病率和持续性的影响。
1993 年佩洛塔斯出生队列的第 7 次随访于 2004 年进行(个体年龄为 10-11 岁)。2008 年 1 月至 8 月,进行了该队列的第 8 次随访。所有仍存活的原始队列个体(当时为 14-15 岁的青少年)都是研究对象。采用国际儿童哮喘和过敏研究(ISAAC)问卷来定义喘息。除了世界卫生组织(WHO)标准定义的肥胖所使用的体重指数(BMI)外,我们还评估了皮褶厚度。
从原始队列中找到了 4349 名个体(85.7%的随访率)。11 岁和 15 岁时胸部喘息的患病率分别为 13.5%(95%CI:12.5%-14.5%)和 12.1%(95%CI:11.1%-13.1%)。两次均有喘息的患病率为 4.5%(95%CI:3.9%-5.1%),喘息的发病率为 7.5%(95%CI:6.7%-8.3%)。在排除各种混杂变量的影响后,11 岁时肥胖个体的 15 岁时喘息患病率比营养良好个体高 50%(RR 1.53;95%CI:1.14-2.05)。11 岁时皮褶厚度越高,15 岁时喘息的患病率越高(p=0.011)。体重状况和皮褶与喘息的发生均无相关性。在控制混杂因素后,11 岁时肥胖个体持续性喘息的风险为 1.82(95%CI:1.30-2.54)。
由于青春期起始时肥胖与哮喘症状持续存在有关,因此预防和治疗肥胖可能会降低不必要的医疗保健费用和疾病负担。