Land Mary-Anne, Webster Jacqui, Christoforou Anthea, Praveen D, Jeffery Paul, Chalmers John, Smith Wayne, Woodward Mark, Barzi Federica, Nowson Caryl, Flood Victoria, Neal Bruce
The George Institute for Global Health, Sydney Medical School, The University of Sydney, Sydney, New South Wales, Australia.
BMJ Open. 2014 Jan 16;4(1):e003720. doi: 10.1136/bmjopen-2013-003720.
The gold standard method for measuring population sodium intake is based on a 24 h urine collection carried out in a random population sample. However, because participant burden is high, response rates are typically low with less than one in four agreeing to provide specimens. At this low level of response it is possible that simply asking for volunteers would produce the same results.
Lithgow, New South Wales, Australia.
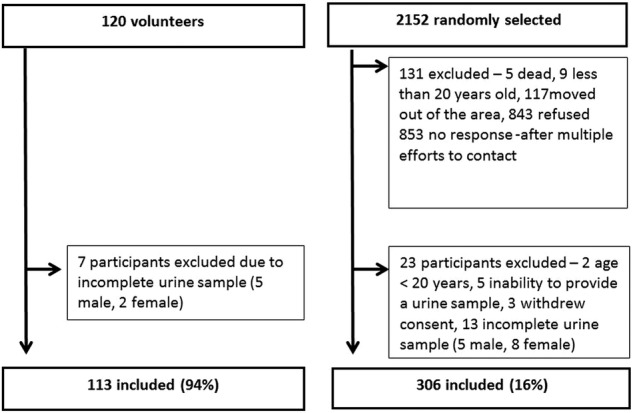
We randomly selected 2152 adults and obtained usable 24 h urine samples from 306 (response rate 16%). Specimens were also collected from a further 113 volunteers. Estimated salt consumption and the costs for each strategy were compared.
The characteristics of the 'random' and 'volunteer' samples were moderately different in mean age 58 (SD 14.6 vs 49(17.7) years, respectively; p<0.001) as well as self-reported alcohol use, tobacco use, history of hypertension and prescription drug use (all p<0.04). Overall crude mean 24 h urinary salt excretion was 8.9(3.6) g/day in the random sample vs 8.5(3.3) g/day for the volunteers (p=0.42). Corresponding age-adjusted and sex-adjusted estimates were 9.2(3.3) and 8.8(3.4) g/day (p=0.29). Estimates for men 10.3(3.8) vs 9.6(3.3) g/day; (p=0.26) and women 7.6(3) vs 7.9(3.2) g/day; (p=0.43) were also similar for the two samples, as was salt excretion across age groups (p=0.72). The cost of obtaining each 24 h urine sample was two times greater for the random compared to volunteer samples ($A62 vs $A31).
The estimated salt consumption derived from the two samples was comparable and was not substantively different to estimates obtained from other surveys. In countries where salt is pervasive and cannot easily be avoided, estimates of consumption obtained from volunteer samples may be valid and less costly.
测量人群钠摄入量的金标准方法是基于对随机抽取的人群样本进行24小时尿液收集。然而,由于参与者负担较重,应答率通常较低,不到四分之一的人同意提供样本。在如此低的应答率下,仅仅招募志愿者可能会产生相同的结果。
澳大利亚新南威尔士州利思戈。
我们随机选取了2152名成年人,从306人(应答率16%)那里获得了可用的24小时尿液样本。还从另外113名志愿者那里收集了样本。比较了每种策略的估计食盐摄入量和成本。
“随机”样本和“志愿者”样本的特征在平均年龄方面存在适度差异,分别为58岁(标准差14.6)和49岁(17.7);p<0.001),在自我报告的饮酒、吸烟、高血压病史和处方药使用方面也存在差异(所有p<0.04)。随机样本中总体24小时尿盐排泄粗均值为8.9(3.6)克/天,志愿者样本为8.5(3.3)克/天(p=0.42)。相应的年龄调整和性别调整估计值分别为9.2(3.3)和8.8(3.4)克/天(p=0.29)。两个样本中男性的估计值分别为10.3(3.8)和9.6(3.3)克/天;(p=0.26),女性为7.6(3)和7.9(3.2)克/天;(p=0.43),各年龄组的盐排泄情况也是如此(p=0.72)。获取每个24小时尿液样本的成本,随机样本是志愿者样本的两倍(62澳元对31澳元)。
从两个样本得出的估计食盐摄入量具有可比性,与其他调查获得的估计值没有实质性差异。在食盐普遍存在且不易避免的国家,从志愿者样本获得的摄入量估计值可能是有效的,且成本较低。