Regional Medical Research Center, Bhubaneswar, Odisha, India.
International Vaccine Institute, Seoul, Republic of Korea.
PLoS Negl Trop Dis. 2014 Feb 6;8(2):e2629. doi: 10.1371/journal.pntd.0002629. eCollection 2014 Feb.
The substantial morbidity and mortality associated with recent cholera outbreaks in Haiti and Zimbabwe, as well as with cholera endemicity in countries throughout Asia and Africa, make a compelling case for supplementary cholera control measures in addition to existing interventions. Clinical trials conducted in Kolkata, India, have led to World Health Organization (WHO)-prequalification of Shanchol, an oral cholera vaccine (OCV) with a demonstrated 65% efficacy at 5 years post-vaccination. However, before this vaccine is widely used in endemic areas or in areas at risk of outbreaks, as recommended by the WHO, policymakers will require empirical evidence on its implementation and delivery costs in public health programs. The objective of the present report is to describe the organization, vaccine coverage, and delivery costs of mass vaccination with a new, less expensive OCV (Shanchol) using existing public health infrastructure in Odisha, India, as a model.
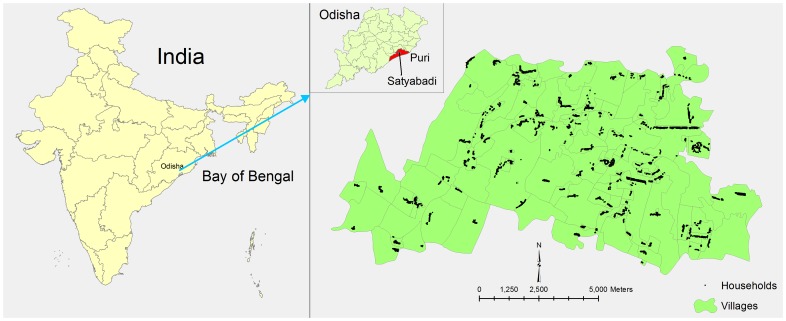
All healthy, non-pregnant residents aged 1 year and above residing in selected villages of the Satyabadi block (Puri district, Odisha, India) were invited to participate in a mass vaccination campaign using two doses of OCV. Prior to the campaign, a de jure census, micro-planning for vaccination and social mobilization activities were implemented. Vaccine coverage for each dose was ascertained as a percentage of the censused population. The direct vaccine delivery costs were estimated by reviewing project expenditure records and by interviewing key personnel.
The mass vaccination was conducted during May and June, 2011, in two phases. In each phase, two vaccine doses were given 14 days apart. Sixty-two vaccination booths, staffed by 395 health workers/volunteers, were established in the community. For the censused population, 31,552 persons (61% of the target population) received the first dose and 23,751 (46%) of these completed their second dose, with a drop-out rate of 25% between the two doses. Higher coverage was observed among females and among 6-17 year-olds. Vaccine cost at market price (about US$1.85/dose) was the costliest item. The vaccine delivery cost was $0.49 per dose or $1.13 per fully vaccinated person.
This is the first undertaken project to collect empirical evidence on the use of Shanchol within a mass vaccination campaign using existing public health program resources. Our findings suggest that mass vaccination is feasible but requires detailed micro-planning. The vaccine and delivery cost is affordable for resource poor countries. Given that the vaccine is now WHO pre-qualified, evidence from this study should encourage oral cholera vaccine use in countries where cholera remains a public health problem.
海地和津巴布韦最近爆发的霍乱疫情以及亚洲和非洲各国的霍乱地方性流行,导致发病率和死亡率居高不下,这有力地证明了除了现有的干预措施之外,还需要采取补充性的霍乱控制措施。在印度加尔各答进行的临床试验,导致世界卫生组织(WHO)将口服霍乱疫苗(OCV)Shanchol 列为合格产品,该疫苗在接种后 5 年内的有效性为 65%。然而,在该疫苗被广泛用于流行地区或有暴发风险的地区之前,如世界卫生组织所建议的那样,决策者将需要有关其在公共卫生规划中的实施和交付成本的经验证据。本报告的目的是描述在印度奥里萨邦的萨蒂亚巴迪(Satyabadi)街区利用现有的公共卫生基础设施,以一种新的、较便宜的 OCV(Shanchol)开展大规模疫苗接种活动的组织、疫苗覆盖率和交付成本,以此作为一种模式。
所有居住在印度奥里萨邦(Odisha)Satyabadi 街区(普里区)选定村庄的 1 岁及以上的健康非孕妇,均被邀请参加使用两剂 OCV 的大规模疫苗接种运动。在运动之前,进行了法定人口普查、疫苗接种微观规划和社会动员活动。通过审查项目支出记录和采访关键人员,确定了每剂疫苗的覆盖率。通过审查项目支出记录和采访关键人员,确定了每剂疫苗的覆盖率。通过审查项目支出记录和采访关键人员,确定了每剂疫苗的覆盖率。直接疫苗接种的交付成本通过审查项目支出记录和采访关键人员来估算。
大规模疫苗接种于 2011 年 5 月至 6 月分两阶段在社区进行。每阶段相隔 14 天接种两剂疫苗。在社区设立了 62 个疫苗接种站,由 395 名卫生工作者/志愿者组成。对于普查人口,有 31,552 人(目标人群的 61%)接种了第一剂疫苗,其中 23,751 人(46%)完成了第二剂疫苗接种,两剂之间的脱落率为 25%。女性和 6-17 岁人群的覆盖率更高。按市场价格(约 1.85 美元/剂)计算,疫苗成本是最昂贵的项目。疫苗接种的交付成本为每剂 0.49 美元或每人完全接种疫苗 1.13 美元。
这是第一个利用现有的公共卫生规划资源开展大规模疫苗接种运动,收集关于使用 Shanchol 的经验证据的项目。我们的研究结果表明,大规模疫苗接种是可行的,但需要详细的微观规划。对于资源匮乏的国家来说,疫苗和交付成本是可以承受的。鉴于该疫苗现已获得世界卫生组织的资格认证,本研究的结果应鼓励在霍乱仍然是公共卫生问题的国家使用口服霍乱疫苗。