Dalianis Tina
Department of Oncology-Pathology, Karolinska Institutet, Cancer Center Karolinska, Karolinska University Hospital, 171 76 Stockholm, Sweden.
Int J Oncol. 2014 Jun;44(6):1799-805. doi: 10.3892/ijo.2014.2355. Epub 2014 Mar 21.
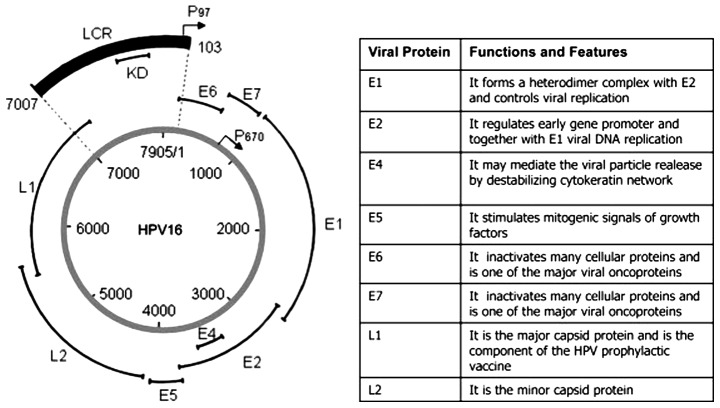
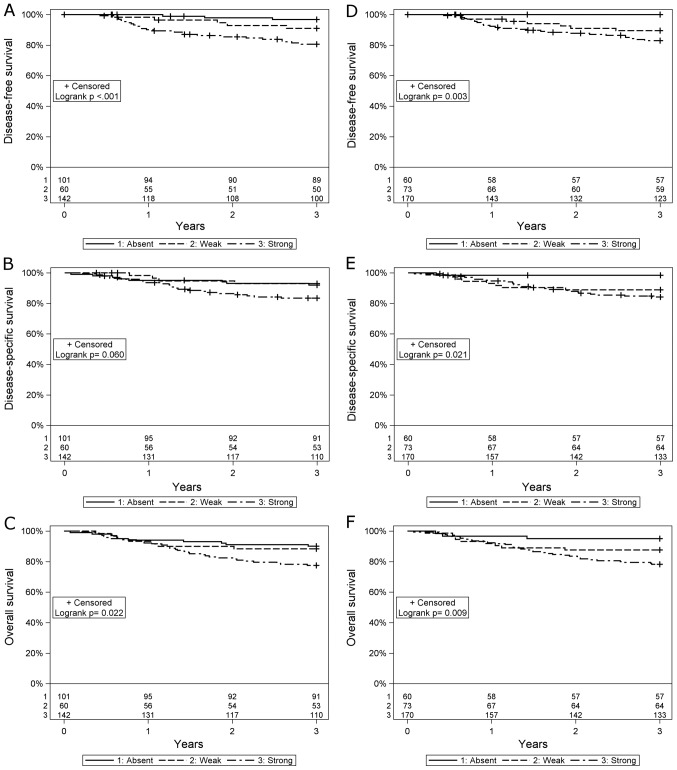
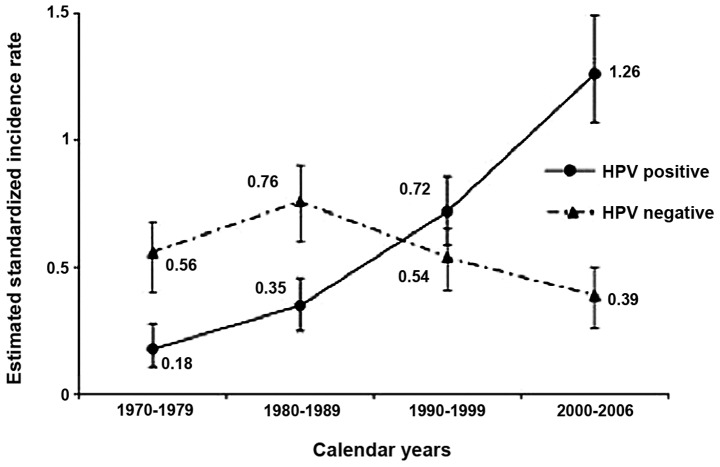
In 2007, the International Agency for Research against Cancer (IARC) recognized human papillomavirus (HPV), especially HPV16, besides smoking and alcohol, as a risk factor for oropharyngeal squamous cell carcinoma (OPSCC), where tonsillar and base of tongue cancer dominate. Moreover, during the past decade, in many Western countries, a sharp rise in the incidence of OPSCC, more specifically of HPV-positive OPSCC has been observed. Notably, patients with HPV-positive OPSCC, where the majority are men, particularly never-smokers have a better clinical outcome than patients with HPV-negative OPSCC and other head neck cancer (roughly 80 vs. 40% disease-free survival with conventional radiotherapy and surgery). This suggests that many patients with HPV-positive OPSCC may not require the more aggressive intensified chemo-radiotherapy given to head neck cancer patients today, and could with somewhat tapered treatment maintain excellent survival, avoiding some of the severe side effects along with intensified treatment. However, before de-intensified treatment is administered additional biomarkers are necessary in combination with HPV-positive status in order to predict and select patients that will respond favorably to therapy. In conclusion, noteworthy issues within this field with an increasing cohort of patients with HPV-positive OPSCC are better-tailored therapy and prevention. Patients with HPV-positive OPSCC, with biomarkers for good response to therapy e.g., low MHC class I, or CD44 expression or high numbers of CD8+ tumor infiltrating lymphocytes, could be included in randomized trials with less severe therapy. Furthermore, possibilities to screen for HPV-positive OPSCC and to vaccinate boys against HPV infection should be further investigated.
2007年,国际癌症研究机构(IARC)认定,除吸烟和饮酒外,人乳头瘤病毒(HPV),尤其是HPV16型,是口咽鳞状细胞癌(OPSCC)的一个风险因素,其中扁桃体癌和舌根癌占主导。此外,在过去十年中,许多西方国家观察到OPSCC的发病率急剧上升,更具体地说是HPV阳性的OPSCC发病率上升。值得注意的是,HPV阳性的OPSCC患者,其中大多数是男性,尤其是从不吸烟者,其临床结局比HPV阴性的OPSCC患者和其他头颈癌患者更好(传统放疗和手术的无病生存率约为80%对40%)。这表明,许多HPV阳性的OPSCC患者可能不需要像如今对头颈癌患者那样进行更积极的强化放化疗,通过某种程度上缩减的治疗就能维持良好的生存率,避免强化治疗带来的一些严重副作用。然而,在进行缩减治疗之前,除了HPV阳性状态外,还需要其他生物标志物来预测和选择对治疗反应良好的患者。总之,在这一领域,随着HPV阳性OPSCC患者群体的增加,值得关注的问题是更精准的治疗和预防。HPV阳性的OPSCC患者,如果有对治疗反应良好的生物标志物,例如低MHC I类分子、CD44表达或大量CD8+肿瘤浸润淋巴细胞,可以纳入治疗强度较低的随机试验。此外,筛查HPV阳性OPSCC以及为男孩接种HPV疫苗的可能性应进一步研究。