Respiratory and Intensive Care Medicine, Cochin Hospital Group, AP-HP, University Paris Descartes, HIA du Val de Grâce 4e C, Paris, France.
BMC Pulm Med. 2014 Apr 2;14:56. doi: 10.1186/1471-2466-14-56.
In Europe, administration of an inhaled corticosteroid (ICS) combined with a long-acting β2 agonist is approved in chronic obstructive pulmonary disease (COPD) patients with a pre-bronchodilator FEV1 < 60% predicted normal, a history of repeated exacerbations, and who have significant symptoms despite regular bronchodilator therapy. Minimal data are available on the use of the fluticasone propionate/salmeterol xinafoate combination (FSC) in the real-life COPD setting and prescription compliance with the licensed specifications.
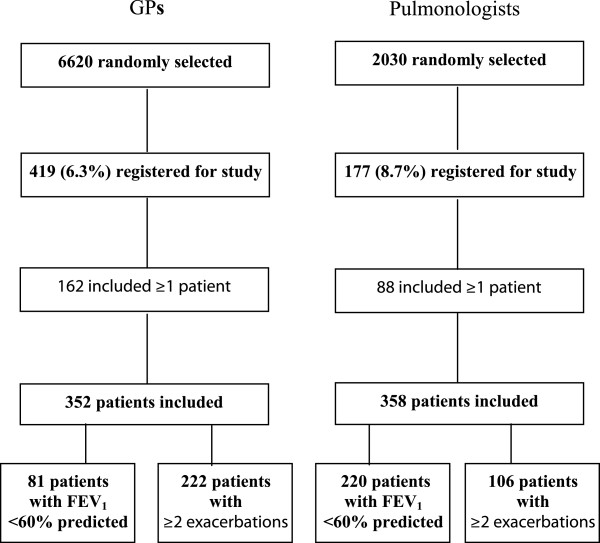
A French observational study was performed to describe the COPD population prescribed with FSC, prescription modalities, and the coherence of prescription practices with the market authorized population. Data were collected for patients initiating FSC treatment (500 μg fluticasone propionate, 50 μg salmeterol, dry powder inhaler) prescribed by a general practitioner (GP) or a pulmonologist, using physician and patient questionnaires.
A total of 710 patients were included, 352 by GPs and 358 by pulmonologists. Mean age was over 60 years, and 70% of patients were male. More than half were retired, and overweight or obese. Approximately half were current smokers and one-third had cardiovascular comorbidities. According to both physician evaluation and GOLD 2006 classification, the majority of patients (>75%) had moderate to very severe COPD. Strict compliance by prescribing physicians with the market-approved population for dry powder inhaler SFC in COPD was low, notably in ICS-naïve patients; all three conditions were fulfilled in less than a quarter of patients with prior ICS and less than 7% of ICS-naïve patients.
Prescription of dry powder inhaler SFC by GPs and pulmonologists has very low conformity with the three conditions defining the licensed COPD population. Prescription practices need to be improved and systematic FEV1 evaluation for COPD diagnosis and treatment management should be emphasized.
在欧洲,对于支气管扩张剂预治疗后第一秒用力呼气量(FEV1)<60%预计值、反复发生加重且即使接受常规支气管扩张剂治疗仍有显著症状的慢性阻塞性肺疾病(COPD)患者,批准了吸入性皮质类固醇(ICS)与长效β2 受体激动剂(LABA)联合用药。关于在真实世界 COPD 环境中使用丙酸氟替卡松/沙美特罗复方制剂(FSC)以及是否符合许可说明书规定的处方顺应性,仅有少量数据。
开展了一项法国观察性研究,旨在描述使用 FSC 治疗的 COPD 患者人群、处方模式以及处方实践与上市许可人群的一致性。使用医生和患者问卷收集了开始接受丙酸氟替卡松/沙美特罗干粉吸入剂(500μg 丙酸氟替卡松,50μg 沙美特罗)治疗的患者数据,这些患者由全科医生(GP)或肺病专家开具处方。
共纳入 710 例患者,其中 352 例由 GP 开具处方,358 例由肺病专家开具处方。平均年龄超过 60 岁,70%的患者为男性。超过一半的患者已退休,超重或肥胖。约一半的患者为当前吸烟者,三分之一的患者合并心血管疾病。根据医生评估和 GOLD 2006 分类,大多数患者(>75%)患有中重度至极重度 COPD。ICS 初治患者处方医生严格遵循干粉吸入器 FSC 治疗 COPD 的上市许可人群的比例较低,三种情况均符合的患者不足四分之一;在既往使用 ICS 的患者中,不到 7%符合条件,而 ICS 初治患者中则不到 1%符合条件。
GP 和肺病专家开具干粉吸入器 FSC 的处方与定义许可 COPD 人群的三个条件非常不符。处方实践需要改进,应强调针对 COPD 诊断和治疗管理的系统 FEV1 评估。