Donovan Nancy J, Amariglio Rebecca E, Zoller Amy S, Rudel Rebecca K, Gomez-Isla Teresa, Blacker Deborah, Hyman Bradley T, Locascio Joseph J, Johnson Keith A, Sperling Reisa A, Marshall Gad A, Rentz Dorene M
Center for Alzheimer Research and Treatment and Department of Neurology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA; Department of Psychiatry, Brigham and Women's Hospital, Harvard Medical School, Boston, MA.
Center for Alzheimer Research and Treatment and Department of Neurology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA; Department of Psychiatry, Brigham and Women's Hospital, Harvard Medical School, Boston, MA; Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA.
Am J Geriatr Psychiatry. 2014 Dec;22(12):1642-51. doi: 10.1016/j.jagp.2014.02.007. Epub 2014 Feb 26.
To examine neuropsychiatric and neuropsychological predictors of progression from normal to early clinical stages of Alzheimer disease (AD).
From a total sample of 559 older adults from the Massachusetts Alzheimer's Disease Research Center longitudinal cohort, 454 were included in the primary analysis: 283 with clinically normal cognition (CN), 115 with mild cognitive impairment (MCI), and 56 with subjective cognitive concerns (SCC) but no objective impairment, a proposed transitional group between CN and MCI. Two latent cognitive factors (memory-semantic, attention-executive) and two neuropsychiatric factors (affective, psychotic) were derived from the Alzheimer's Disease Centers' Uniform Data Set neuropsychological battery and Neuropsychiatric Inventory brief questionnaire. Factors were analyzed as predictors of time to progression to a worse diagnosis using a Cox proportional hazards regression model with backward elimination. Covariates included baseline diagnosis, gender, age, education, prior depression, antidepressant medication, symptom duration, and interaction terms.
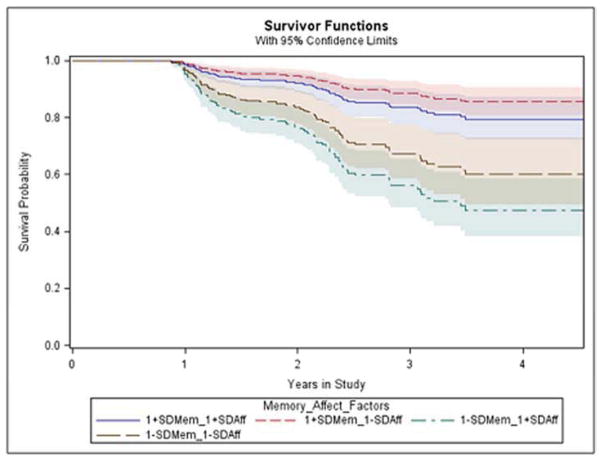
Higher/better memory-semantic factor score predicted lower hazard of progression (hazard ratio [HR] = 0.4 for 1 standard deviation [SD] increase, p <0.0001), and higher/worse affective factor score predicted higher hazard (HR = 1.3 for one SD increase, p = 0.01). No other predictors were significant in adjusted analyses. Using diagnosis as a sole predictor of transition to MCI, the SCC diagnosis carried a fourfold risk of progression compared with CN (HR = 4.1, p <0.0001).
These results identify affective and memory-semantic factors as significant predictors of more rapid progression from normal to early stages of cognitive decline and highlight the subgroup of cognitively normal elderly with SCC as those with elevated risk of progression to MCI.
研究从正常状态进展至阿尔茨海默病(AD)临床早期阶段的神经精神及神经心理学预测因素。
在马萨诸塞州阿尔茨海默病研究中心纵向队列的559名老年人总样本中,454人纳入主要分析:283人认知功能临床正常(CN),115人轻度认知障碍(MCI),56人有主观认知问题(SCC)但无客观损害,这是一个介于CN和MCI之间的拟议过渡组。从阿尔茨海默病中心统一数据集神经心理成套测验和神经精神科问卷简表中得出两个潜在认知因素(记忆语义、注意力执行)和两个神经精神因素(情感、精神病性)。使用带有向后剔除的Cox比例风险回归模型,将这些因素作为进展至更差诊断时间的预测因素进行分析。协变量包括基线诊断、性别、年龄、教育程度、既往抑郁史、抗抑郁药物治疗、症状持续时间及交互项。
较高/较好的记忆语义因素得分预测进展风险较低(1个标准差[SD]增加时风险比[HR]=0.4,p<0.0OO1),较高/较差的情感因素得分预测进展风险较高(1个SD增加时HR=1.3,p=0.01)。在调整分析中,无其他预测因素具有显著性。以诊断作为向MCI转变的唯一预测因素,SCC诊断进展风险是CN的4倍(HR=4.1,p<0.0001)。
这些结果确定情感和记忆语义因素是从正常快速进展至认知衰退早期阶段的显著预测因素,并强调有SCC的认知正常老年人亚组是进展至MCI风险升高的人群。