Murhekar Manoj V, Ahmad Mohammad, Shukla Hemant, Abhishek Kunwar, Perry Robert T, Bose Anindya S, Shimpi Rahul, Kumar Arun, Kaliaperumal Kanagasabai, Sethi Raman, Selvaraj Vadivoo, Kamaraj Pattabi, Routray Satyabrata, Das Vidya Nand, Menabde Nata, Bahl Sunil
National Institute of Epidemiology, ICMR, Chennai, India.
World Health Organization- Country Office for India, National Polio Surveillance Project, New Delhi, India.
PLoS One. 2014 May 13;9(5):e96668. doi: 10.1371/journal.pone.0096668. eCollection 2014.
Updated estimates of measles case fatality rates (CFR) are critical for monitoring progress towards measles elimination goals. India accounted for 36% of total measles deaths occurred globally in 2011. We conducted a retrospective cohort study to estimate measles CFR and identify the risk factors for measles death in Bihar-one of the north Indian states historically known for its low vaccination coverage.
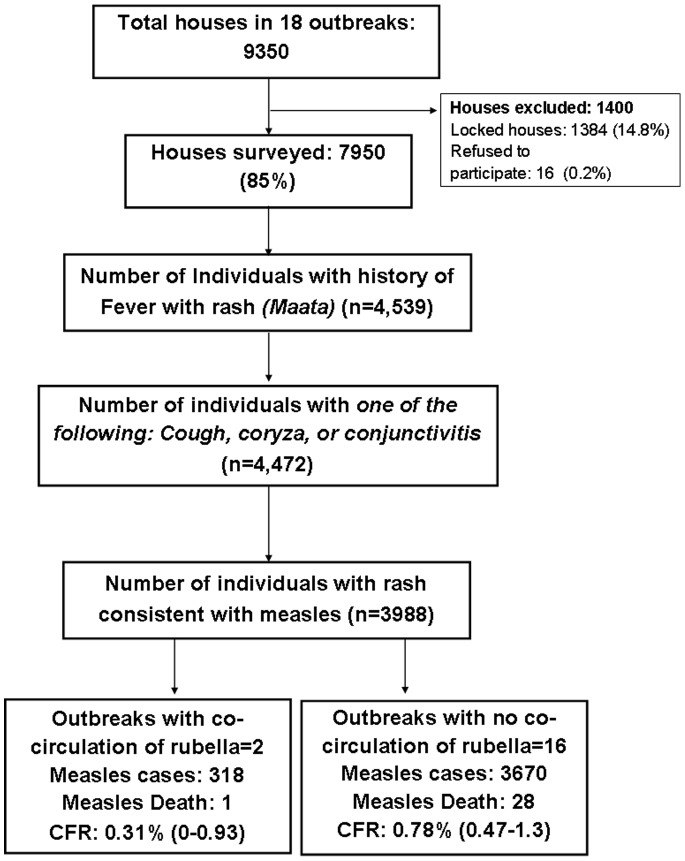
We systematically selected 16 of the 31 laboratory-confirmed measles outbreaks occurring in Bihar during 1 October 2011 to 30 April 2012. All households of the villages/urban localities affected by these outbreaks were visited to identify measles cases and deaths. We calculated CFR and used multivariate analysis to identify risk factors for measles death.
The survey found 3670 measles cases and 28 deaths (CFR: 0.78, 95% confidence interval: 0.47-1.30). CFR was higher among under-five children (1.22%) and children belonging to scheduled castes/tribes (SC/ST, 1.72%). On multivariate analysis, independent risk factors associated with measles death were age <5 years, SC/ST status and non-administration of vitamin A during illness. Outbreaks with longer interval between the occurrence of first case and notification of the outbreak also had a higher rate of deaths.
Measles CFR in Bihar was low. To further reduce case fatality, health authorities need to ensure that SC/ST are targeted by the immunization programme and that outbreak investigations target for vitamin A treatment of cases in high risk groups such as SC/ST and young children and ensure regular visits by health-workers in affected villages to administer vitamin A to new cases.
更新麻疹病死率(CFR)的估计值对于监测消除麻疹目标的进展情况至关重要。2011年,印度的麻疹死亡病例占全球麻疹死亡总数的36%。我们开展了一项回顾性队列研究,以估计比哈尔邦(印度北部一个历史上以低疫苗接种覆盖率闻名的邦)的麻疹病死率,并确定麻疹死亡的危险因素。
我们系统地选取了2011年10月1日至2012年4月30日期间在比哈尔邦发生的31起实验室确诊的麻疹疫情中的16起。走访了受这些疫情影响的村庄/城市地区的所有家庭,以确定麻疹病例和死亡情况。我们计算了病死率,并使用多变量分析来确定麻疹死亡的危险因素。
调查发现3670例麻疹病例和28例死亡(病死率:0.78,95%置信区间:0.47 - 1.30)。五岁以下儿童(1.22%)以及在册种姓/部落(SC/ST,1.72%)的儿童病死率更高。多变量分析显示,与麻疹死亡相关的独立危险因素为年龄小于5岁、SC/ST身份以及患病期间未补充维生素A。首例病例出现与疫情通报之间间隔时间较长的疫情,其死亡率也较高。
比哈尔邦的麻疹病死率较低。为进一步降低病死率,卫生当局需要确保免疫规划针对SC/ST群体,疫情调查要针对SC/ST和幼儿等高风险群体的病例进行维生素A治疗,并确保卫生工作者定期走访受影响村庄,为新病例补充维生素A。