Ahmed Tanvir, Lucas Henry, Khan Azfar Sadun, Islam Rubana, Bhuiya Abbas, Iqbal Mohammad
Centre for Equity and Heath Systems, International Center for Diarrhoeal Disease Research, Bangladesh (ICDDR,B)68, ShaheedTajuddin Ahmed Sarani, Mohakhali, Dhaka 1212, Bangladesh.
BMC Health Serv Res. 2014 Jun 16;14:260. doi: 10.1186/1472-6963-14-260.
The health system of Bangladesh is haunted by challenges of accessibility and affordability. Despite impressive gains in many health indicators, recent evidence has raised concerns regarding the utilization, quality and equity of healthcare. In the context of new and unfamiliar public health challenges including high population density and rapid urbanization, eHealth and mHealth are being promoted as a route to cost-effective, equitable and quality healthcare in Bangladesh. The aim of this paper is to highlight such initiatives and understand their true potential.
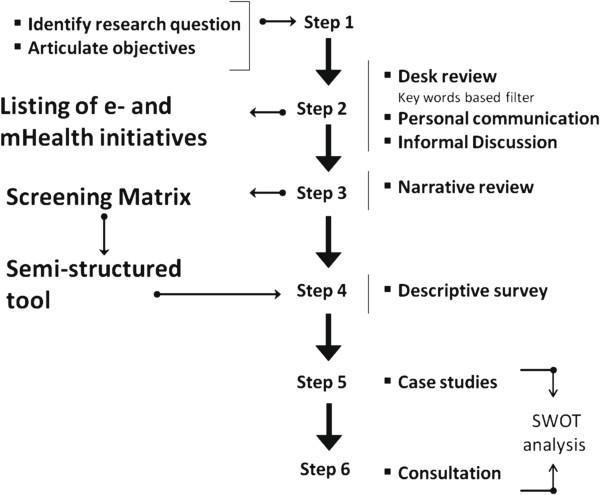
This scoping study applies a combination of research tools to explore 26 eHealth and mHealth initiatives in Bangladesh. A screening matrix was developed by modifying the framework of Arksey & O'Malley, further complemented by case study and SWOT analysis to identify common traits among the selected interventions. The WHO health system building blocks approach was then used for thematic analysis of these traits.
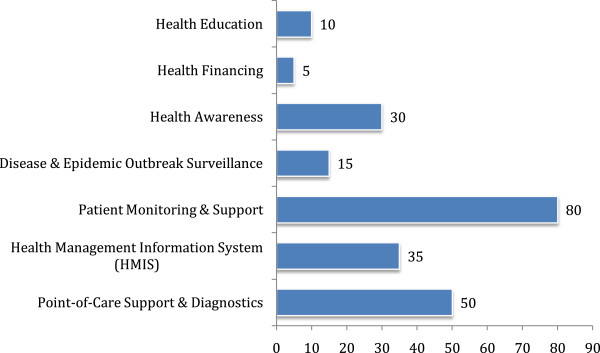
Findings suggest that most eHealth and mHealth initiatives have proliferated within the private sector, using mobile phones. The most common initiatives include tele-consultation, prescription and referral. While a minority of projects have a monitoring and evaluation framework, less than a quarter have undertaken evaluation. Most of the initiatives use a health management information system (HMIS) to monitor implementation. However, these do not provide for effective sharing of information and interconnectedness among the various actors. There are extremely few individuals with eHealth training in Bangladesh and there is a strong demand for capacity building and experience sharing, especially for implementation and policy making. There is also a lack of research evidence on how to design interventions to meet the needs of the population and on potential benefits.
This study concludes that Bangladesh needs considerable preparation and planning to sustain eHealth and mHealth initiatives successfully. Additional formative and operational research is essential to explore the true potential of the technology. Frameworks for regulation in regards to eHealth governance should be the aim of future research on the integration of eHealth and mHealth into the Bangladesh health system.
孟加拉国的卫生系统面临着可及性和可负担性方面的挑战。尽管在许多卫生指标上取得了令人瞩目的进展,但最近的证据引发了人们对医疗保健利用、质量和公平性的担忧。在包括高人口密度和快速城市化在内的新的、不熟悉的公共卫生挑战背景下,电子健康(eHealth)和移动健康(mHealth)被作为在孟加拉国实现具有成本效益、公平且高质量医疗保健的途径加以推广。本文旨在突出此类举措并了解其真正潜力。
这项范围界定研究运用多种研究工具,对孟加拉国的26项电子健康和移动健康举措进行探索。通过修改阿克西和奥马利的框架开发了一个筛选矩阵,并辅以案例研究和SWOT分析,以确定所选干预措施的共同特征。然后使用世界卫生组织卫生系统构建模块方法对这些特征进行主题分析。
研究结果表明,大多数电子健康和移动健康举措在私营部门内激增,利用手机开展。最常见的举措包括远程会诊、开处方和转诊。虽然少数项目有监测和评估框架,但不到四分之一的项目进行了评估。大多数举措使用卫生管理信息系统(HMIS)来监测实施情况。然而,这些系统并未实现各行为主体之间信息的有效共享和互联互通。孟加拉国接受电子健康培训的人员极少,对能力建设和经验分享,尤其是实施和政策制定方面的需求强烈。关于如何设计干预措施以满足民众需求以及潜在益处,也缺乏研究证据。
本研究得出结论,孟加拉国需要进行大量准备和规划,以成功维持电子健康和移动健康举措。开展更多的形成性研究和操作性研究对于探索该技术的真正潜力至关重要。关于电子健康治理的监管框架应成为未来将电子健康和移动健康融入孟加拉国卫生系统研究的目标。