Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil.
Braz J Otorhinolaryngol. 2014 May-Jun;80(3):202-7. doi: 10.1016/j.bjorl.2014.02.001.
Establishing a diagnosis in patients with olfactory disturbances has always been challenging for physicians.One reason for this is the rarity of some of the diseases that affect this sense, such as Kallmann's syndrome and post-viral olfactory loss.
To identify the major causes of olfactory disturbances and to describe the diagnostic evaluation in outpatients attended to at an ambulatory clinic specialized in olfaction disorders.
A retrospective analysis was performed in outpatients with primary olfactory complaint attended to between June 1, 2011 and September 30, 2013 in a center specialized in olfactory disorders. Patient history, nasofibroscopy, and the University of Pennsylvania Smell Identification Test (UPSIT) comprised the examination.
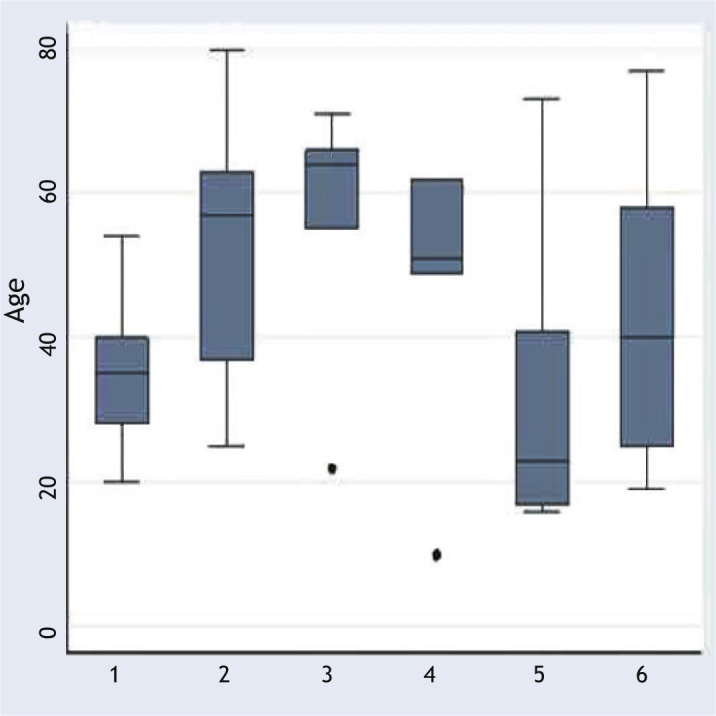
Sixty-two patients were evaluated. The major causes were chronic rhinosinusitis (31%); rhinitis, primarily the allergic type (19%); post-viral olfactory loss (13%); and post-traumatic loss (8%). UPSIT scores were statistically different among different etiologies (p = 0.01).
The major diagnoses that should be part of the physician assessment when a patient complains of olfactory disturbance are chronic rhinosinusitis with and without polyps, allergic rhinitis, post-viral olfactory loss, and post-traumatic loss.
对于医生来说,诊断嗅觉障碍患者的疾病一直具有挑战性。原因之一是一些影响嗅觉的疾病比较罕见,如 Kallmann 综合征和病毒性嗅觉丧失。
确定嗅觉障碍的主要病因,并描述在嗅觉障碍门诊就诊的门诊患者的诊断评估。
对 2011 年 6 月 1 日至 2013 年 9 月 30 日在嗅觉障碍中心就诊的有原发性嗅觉主诉的门诊患者进行回顾性分析。检查包括患者病史、鼻内窥镜检查和宾夕法尼亚大学嗅觉识别测试(UPSIT)。
共评估了 62 名患者。主要病因是慢性鼻-鼻窦炎(31%);鼻炎,主要是过敏性(19%);病毒性嗅觉丧失(13%)和创伤后嗅觉丧失(8%)。不同病因的 UPSIT 评分存在统计学差异(p=0.01)。
当患者抱怨嗅觉障碍时,医生评估应包括慢性鼻-鼻窦炎伴或不伴息肉、过敏性鼻炎、病毒性嗅觉丧失和创伤后嗅觉丧失等主要诊断。