Department of Child and Adolescent Mental Health, National Institute of Mental Health, National Center of Neurology and Psychiatry, 4-1-1 Ogawa-Higashi, Kodaira 187-8553, Tokyo, Japan.
BMC Psychiatry. 2014 Nov 18;14:302. doi: 10.1186/s12888-014-0302-z.
Recently great attention has been paid to the still unmet clinical needs of most adults with autism spectrum disorder (ASD) who live in the community, an increasing number of whom visit psychiatric clinics to seek accurate diagnosis and treatment of concurrent psychiatric symptoms. However, different from the case of children diagnosed with ASD in childhood, it is difficult in adults to identify the ASD symptoms underlying psychopathology and to differentiate ASD from other psychiatric disorders in general psychiatric practice. This study aimed to verify the utility of the Social Responsiveness Scale-Adult version (SRS-A), a quantitative measure for identifying ASD symptoms, in non-clinical and clinical adult populations in Japan.
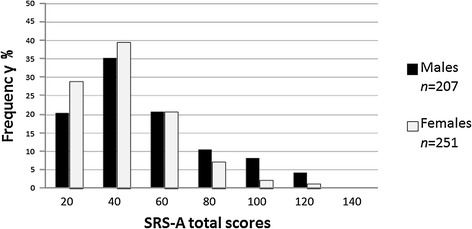
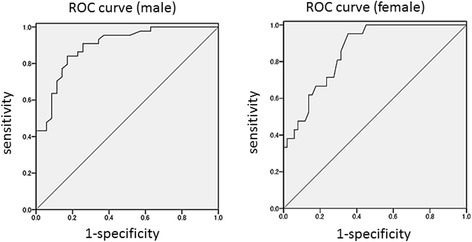
The total sample aged 19 to 59 years consisted of a non-clinical population (n =592) and clinical population with and without ASD (n =142). We examined score distributions of the Japanese version of the scale, and the effects of gender, age, and rater on the distribution. We analyzed factor structure and internal consistency in the non-clinical normative sample, and analyzed convergent, divergent, and discriminative validities in the clinical sample. We applied receiver operator characteristic (ROC) analysis to determine optimal cutoff scores discriminating the ASD clinical population from the non-ASD clinical population.
The score distributed continuously, which replicated findings in children. For non-clinical adults, except in men aged 19 to 24 years, we found no or few gender, age, or rater effects. Both single- and two-factor models were supported for adults. Total SRS-A scores demonstrated high internal consistency and capably discriminated adults with ASD from those with non-ASD psychiatric disorders such as major depressive disorder, schizophrenia, and bipolar disorder with an overlap across diagnoses. Moderate to high correlations of the SRS-A with other-rated ASD measures indicated sufficient convergent validity. Based on the ROC analysis, we recommend cutoff points by gender for use in clinical settings.
This study provides additional supportive evidence that the Japanese version SRS-A can reliably and validly measure ASD symptoms in non-clinical and clinical adult populations, and thus can serve as a useful tool for ASD research as well as for secondary screening in Japanese adults.
最近,人们越来越关注社区中大多数自闭症谱系障碍(ASD)成年人的未满足的临床需求,越来越多的成年人到精神病诊所寻求准确的诊断和治疗并发的精神症状。然而,与儿童时期被诊断为 ASD 的情况不同,在普通精神病学实践中,很难识别精神病理学中的 ASD 症状,并将 ASD 与其他精神障碍区分开来。本研究旨在验证社会反应量表成人版(SRS-A)在日本非临床和临床成年人群中的有效性,该量表是一种用于识别 ASD 症状的定量测量工具。
总样本年龄为 19 至 59 岁,包括非临床人群(n=592)和伴有或不伴有 ASD 的临床人群(n=142)。我们检查了该量表的日本版本的分数分布情况,并考察了性别、年龄和评分者对分布的影响。我们在非临床常模样本中分析了因子结构和内部一致性,并在临床样本中分析了收敛性、发散性和判别有效性。我们应用接受者操作特征(ROC)分析来确定区分 ASD 临床人群和非 ASD 临床人群的最佳截断分数。
分数呈连续分布,与儿童的研究结果一致。对于非临床成年人,除了 19 至 24 岁的男性外,我们发现性别、年龄或评分者几乎没有或没有影响。成人支持单因子和双因子模型。SRS-A 总分具有较高的内部一致性,能够将 ASD 成年人与其他精神障碍(如重度抑郁症、精神分裂症和双相情感障碍)区分开来,而不同诊断之间存在重叠。SRS-A 与其他评定的 ASD 测量指标的中等至高度相关性表明具有足够的收敛效度。基于 ROC 分析,我们建议根据性别推荐用于临床的截断点。
本研究提供了额外的支持证据,表明日本版 SRS-A 可以可靠有效地测量非临床和临床成年人群中的 ASD 症状,因此可以作为 ASD 研究以及日本成年人二级筛查的有用工具。