Sharp Tyler M, Roth Nicole M, Torres Jomil, Ryff Kyle R, Pérez Rodríguez Nicole M, Mercado Chanis, Pilar Diaz Padró Maria Del, Ramos Maria, Phillips Raina, Lozier Matthew, Arriola Carmen S, Johansson Michael, Hunsperger Elizabeth, Muñoz-Jordán Jorge L, Margolis Harold S, García Brenda Rivera
MMWR Morb Mortal Wkly Rep. 2014 Dec 5;63(48):1121-8.
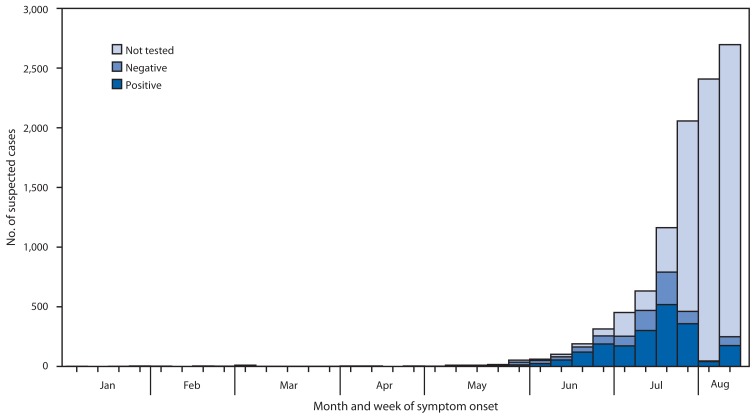
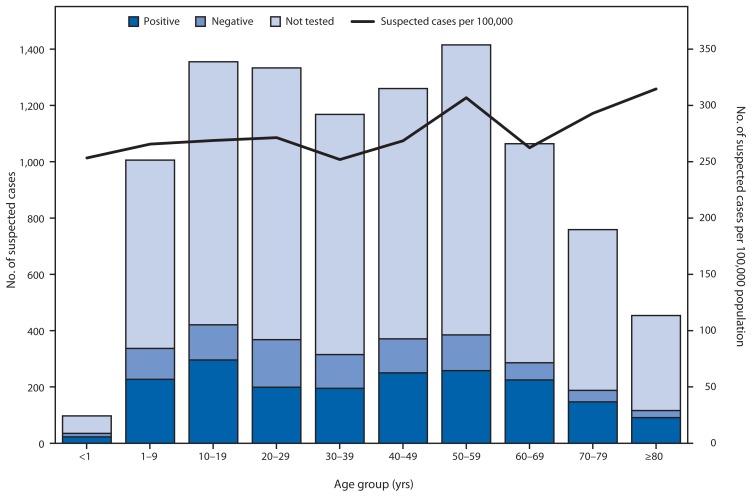
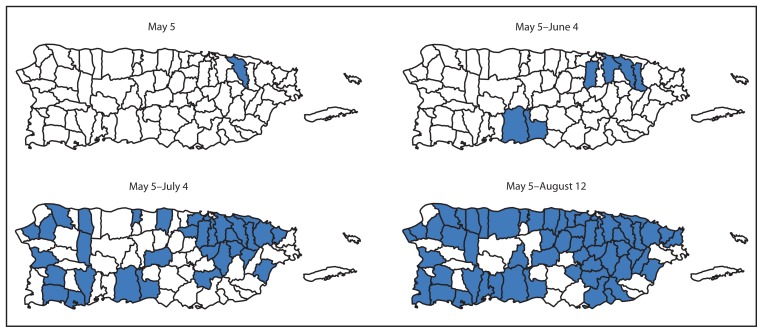
Chikungunya and dengue are mosquito-borne, viral, acute febrile illnesses that can be difficult to distinguish clinically. Whereas dengue is endemic in many countries in the Caribbean and the Americas, the first locally acquired chikungunya case in the Western Hemisphere was reported from the Caribbean island of St. Martin in December 2013 and was soon followed by cases in many parts of the region. In January 2014, the Puerto Rico Department of Health (PRDH) and CDC initiated chikungunya surveillance by building on an existing passive dengue surveillance system. To assess the extent of chikungunya in Puerto Rico, the severity of illnesses, and the health care-seeking behaviors of residents, PRDH and CDC analyzed data from passive surveillance and investigations conducted around the households of laboratory-positive chikungunya patients. Passive surveillance indicated that the first locally acquired, laboratory-positive chikungunya case in Puerto Rico was in a patient with illness onset on May 5, 2014. By August 12, a total of 10,201 suspected chikungunya cases (282 per 100,000 residents) had been reported. Specimens from 2,910 suspected cases were tested, and 1,975 (68%) were positive for chikungunya virus (CHIKV) infection. Four deaths were reported. The household investigations found that, of 250 participants, 70 (28%) tested positive for current or recent CHIKV infection, including 59 (84%) who reported illness within the preceding 3 months. Of 25 laboratory-positive participants that sought medical care, five (20%) were diagnosed with chikungunya and two (8%) were reported to PRDH. These investigative efforts indicated that chikungunya cases were underrecognized and underreported, prompting PRDH to conduct information campaigns to increase knowledge of the disease among health care professionals and the public. PRDH and CDC recommended that health care providers manage suspected chikungunya cases as they do dengue because of the similarities in symptoms and increased risk for complications in dengue patients that are not appropriately managed. Residents of and travelers to the tropics can minimize their risk for both chikungunya and dengue by taking standard measures to avoid mosquito bites.
基孔肯雅热和登革热是由蚊子传播的病毒性急性发热疾病,临床上很难区分。登革热在加勒比地区和美洲的许多国家流行,而西半球首例本地感染的基孔肯雅热病例于2013年12月在加勒比海的圣马丁岛报告,随后该地区许多地方也出现了病例。2014年1月,波多黎各卫生部(PRDH)和美国疾病控制与预防中心(CDC)在现有的被动登革热监测系统基础上启动了基孔肯雅热监测。为评估基孔肯雅热在波多黎各的流行程度、疾病严重程度以及居民寻求医疗服务的行为,PRDH和CDC分析了被动监测数据以及围绕实验室确诊的基孔肯雅热患者家庭展开的调查数据。被动监测表明,波多黎各首例本地感染、实验室确诊的基孔肯雅热病例是一名于2014年5月5日发病的患者。截至8月12日,共报告了10201例疑似基孔肯雅热病例(每10万居民中有282例)。对2910例疑似病例的样本进行了检测,其中1975例(68%)基孔肯雅病毒(CHIKV)感染呈阳性。报告了4例死亡病例。家庭调查发现,在250名参与者中,70例(28%)当前或近期CHIKV感染检测呈阳性,其中59例(84%)报告在过去3个月内患病。在寻求医疗服务的25例实验室确诊参与者中,5例(20%)被诊断为基孔肯雅热,2例(8%)报告给了PRDH。这些调查结果表明,基孔肯雅热病例未得到充分认识和报告,促使PRDH开展宣传活动,以提高医疗保健专业人员和公众对该疾病的认识。PRDH和CDC建议,由于症状相似且未得到妥善治疗的登革热患者出现并发症的风险增加,医疗保健提供者应像处理登革热病例一样处理疑似基孔肯雅热病例。热带地区的居民和旅行者可以通过采取标准措施避免蚊虫叮咬,将感染基孔肯雅热和登革热的风险降至最低。