Bloch Danielle, Roth Nicole M, Caraballo Elba V, Muñoz-Jordan Jorge, Hunsperger Elizabeth, Rivera Aidsa, Pérez-Padilla Janice, Rivera Garcia Brenda, Sharp Tyler M
Dengue Branch, Division of Vector-Borne Diseases, Centers for Disease Control and Prevention, San Juan, Puerto Rico.
Department of Epidemiology of Microbial Disease, Yale School of Public Health, New Haven, Connecticut.
PLoS Negl Trop Dis. 2016 Oct 20;10(10):e0005075. doi: 10.1371/journal.pntd.0005075. eCollection 2016 Oct.
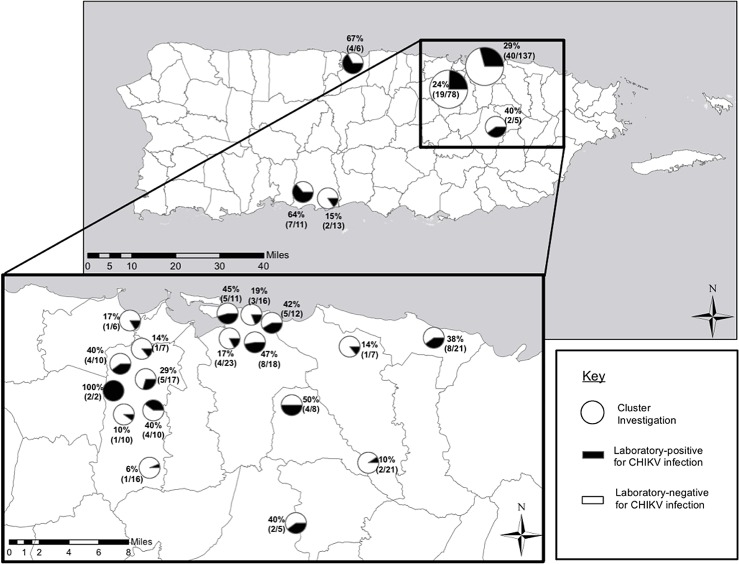
Chikungunya virus (CHIKV) is transmitted by Aedes species mosquitoes and is the cause of an acute febrile illness characterized by potentially debilitating arthralgia. After emerging in the Caribbean in late 2013, the first locally-acquired case reported to public health authorities in Puerto Rico occurred in May 2014. During June-August 2014, household-based cluster investigations were conducted to identify factors associated with infection, development of disease, and case reporting.
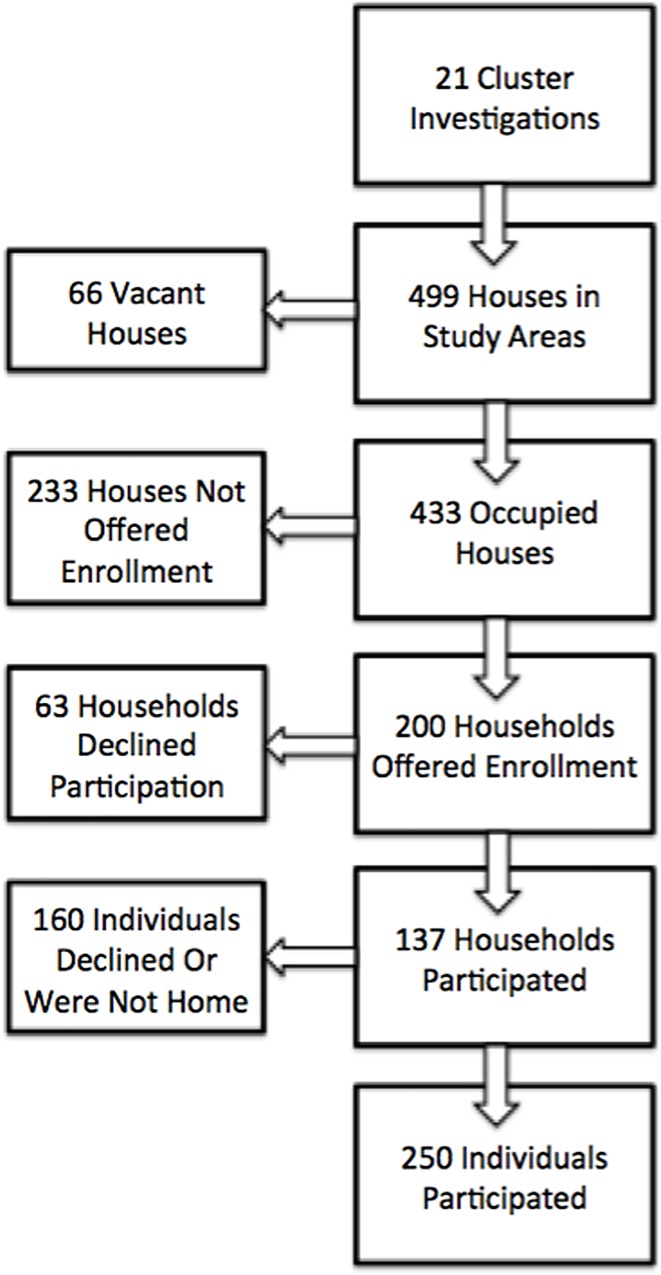
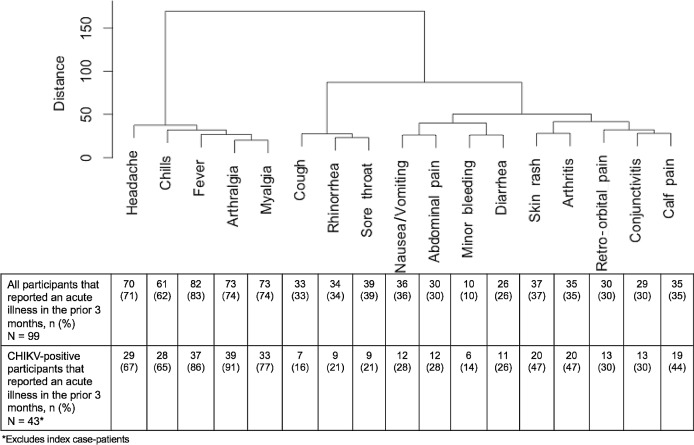
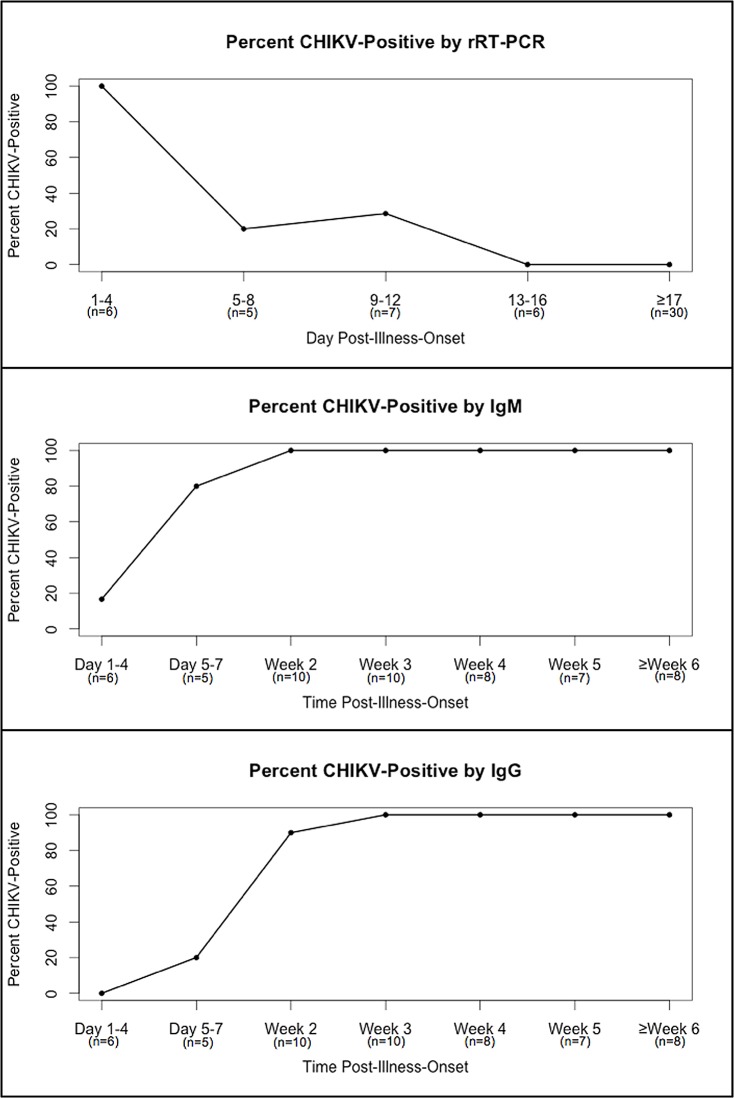
METHODOLOGY/PRINCIPAL FINDINGS: Residents of households within a 50-meter radius of the residence of laboratory-positive chikungunya cases that had been reported to Puerto Rico Department of Health (PRDH) were offered participation in the investigation. Participants provided a serum specimen and answered a questionnaire that collected information on demographic factors, household characteristics, recent illnesses, healthcare seeking behaviors, and clinical diagnoses. Current CHIKV infection was identified by rRT-PCR, and recent CHIKV infection was defined by detection of either anti-CHIKV IgM or IgG antibody. Among 250 participants, 74 (30%) had evidence of CHIKV infection, including 12 (5%) with current and 62 (25%) with recent CHIKV infection. All specimens from patients with CHIKV infection that were collected within four days, two weeks, and three weeks of illness onset were positive by RT-PCR, IgM ELISA, and IgG ELISA, respectively. Reporting an acute illness in the prior three months was strongly associated with CHIKV infection (adjusted odds ratio [aOR] = 21.6, 95% confidence interval [CI]: 9.24-50.3). Use of air conditioning (aOR = 0.50, 95% CI = 0.3-0.9) and citronella candles (aOR = 0.4, 95% CI = 0.1-0.9) were associated with protection from CHIKV infection. Multivariable analysis indicated that arthralgia (aOR = 51.8, 95% CI = 3.8-700.8) and skin rash (aOR = 14.2, 95% CI = 2.4-84.7) were strongly associated with CHIKV infection. Hierarchical cluster analysis of signs and symptoms reported by CHIKV-infected participants demonstrated that fever, arthralgia, myalgia, headache, and chills tended to occur simultaneously. Rate of symptomatic CHIKV infection (defined by arthralgia with fever or skin rash) was 62.5%. Excluding index case-patients, 22 (63%) participants with symptomatic CHIKV infection sought medical care, of which 5 (23%) were diagnosed with chikungunya and 2 (9%) were reported to PRDH.
CONCLUSIONS/SIGNIFICANCE: This investigation revealed high rates of CHIKV infection among household members and neighbors of chikungunya patients, and that behavioral interventions such as use of air conditioning were associated with prevention of CHIKV infection. Nearly two-thirds of patients with symptomatic CHIKV infection sought medical care, of which less than one-quarter were reportedly diagnosed with chikungunya and one-in-ten were reported to public health authorities. These findings emphasize the need for point-of-care rapid diagnostic tests to optimize identification and reporting of chikungunya patients.
基孔肯雅病毒(CHIKV)通过伊蚊传播,是一种急性发热疾病的病原体,其特征为可能使人衰弱的关节痛。2013年末在加勒比地区出现后,波多黎各向公共卫生当局报告的首例本地感染病例发生于2014年5月。在2014年6月至8月期间,开展了基于家庭的聚集性调查,以确定与感染、疾病发展及病例报告相关的因素。
方法/主要发现:向居住在波多黎各卫生部(PRDH)报告的实验室确诊基孔肯雅病例住所半径50米范围内家庭的居民提供参与调查的机会。参与者提供一份血清标本,并回答一份问卷,问卷收集有关人口统计学因素、家庭特征、近期疾病、就医行为及临床诊断的信息。通过逆转录实时聚合酶链反应(rRT-PCR)鉴定当前的CHIKV感染,通过检测抗CHIKV IgM或IgG抗体定义近期的CHIKV感染。在250名参与者中,74人(30%)有CHIKV感染证据,包括12人(5%)为当前感染,62人(25%)为近期感染。CHIKV感染患者在发病后4天、2周和3周内采集的所有标本分别通过RT-PCR、IgM酶联免疫吸附测定(ELISA)和IgG ELISA检测均呈阳性。报告前三个月内有急性疾病与CHIKV感染密切相关(校正比值比[aOR]=21.6,95%置信区间[CI]:9.24 - 50.3)。使用空调(aOR = 0.50,95% CI = 0.3 - 0.9)和香茅蜡烛(aOR = 0.4,95% CI = 0.1 - 0.9)与预防CHIKV感染相关。多变量分析表明,关节痛(aOR = 51.8,95% CI = 3.8 - 700.8)和皮疹(aOR = 14.2,95% CI = 2.4 - 84.7)与CHIKV感染密切相关。对CHIKV感染参与者报告的体征和症状进行的分层聚类分析表明,发热、关节痛、肌痛、头痛和寒战往往同时出现。有症状的CHIKV感染率(定义为伴有发热或皮疹的关节痛)为62.5%。排除索引病例患者后,22名(63%)有症状的CHIKV感染参与者寻求医疗护理,其中5人(23%)被诊断为基孔肯雅热,2人(9%)向PRDH报告。
结论/意义:本次调查揭示了基孔肯雅热患者家庭成员和邻居中CHIKV感染率较高,并表明使用空调等行为干预措施与预防CHIKV感染相关。近三分之二有症状的CHIKV感染患者寻求医疗护理,其中据报告不到四分之一被诊断为基孔肯雅热,十分之一向公共卫生当局报告。这些发现强调了即时检验快速诊断试验对于优化基孔肯雅热患者识别和报告的必要性。