Coslovsky Michael, Takala Jukka, Exadaktylos Aristomenis K, Martinolli Luca, Merz Tobias M
Clinical Trials Unit, Institute of Social and Preventive Medicine, University of Bern, 3010, Bern, Switzerland.
Intensive Care Med. 2015 Jun;41(6):1029-36. doi: 10.1007/s00134-015-3737-x. Epub 2015 Mar 20.
Rapid assessment and intervention is important for the prognosis of acutely ill patients admitted to the emergency department (ED). The aim of this study was to prospectively develop and validate a model predicting the risk of in-hospital death based on all available information available at the time of ED admission and to compare its discriminative performance with a non-systematic risk estimate by the triaging first health-care provider.
Prospective cohort analysis based on a multivariable logistic regression for the probability of death.
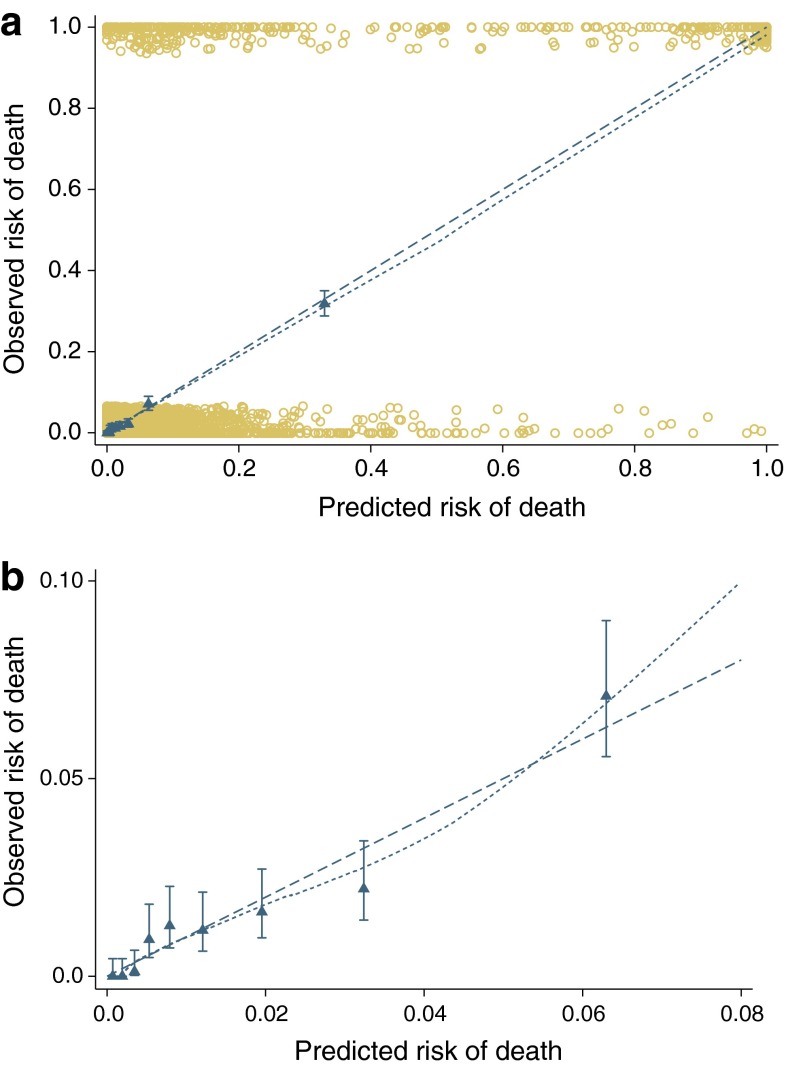
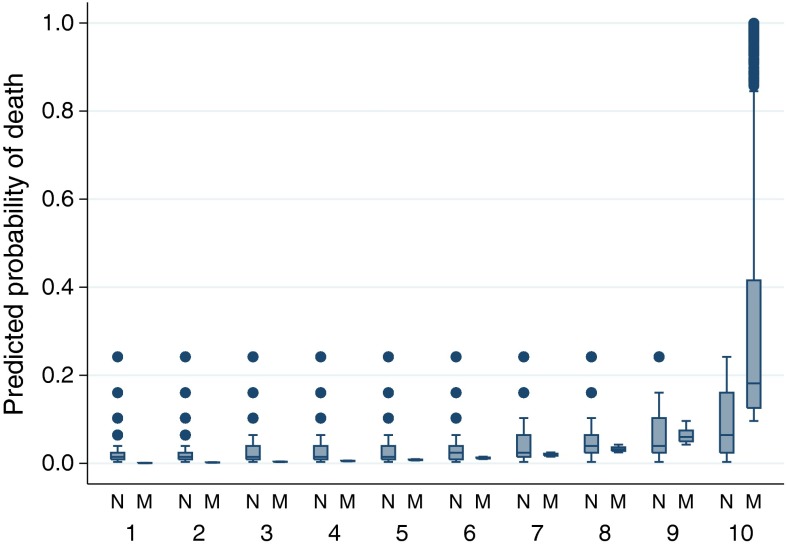
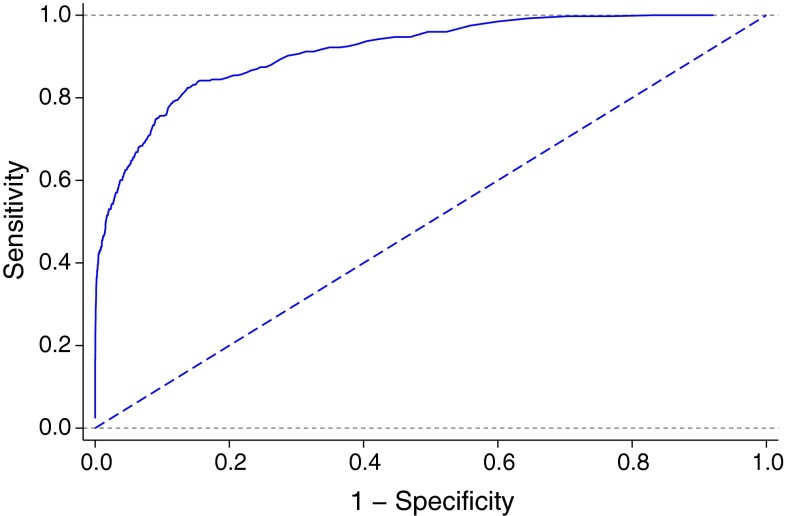
A total of 8,607 consecutive admissions of 7,680 patients admitted to the ED of a tertiary care hospital were analysed. Most frequent APACHE II diagnostic categories at the time of admission were neurological (2,052, 24%), trauma (1,522, 18%), infection categories [1,328, 15%; including sepsis (357, 4.1%), severe sepsis (249, 2.9%), septic shock (27, 0.3%)], cardiovascular (1,022, 12%), gastrointestinal (848, 10%) and respiratory (449, 5%). The predictors of the final model were age, prolonged capillary refill time, blood pressure, mechanical ventilation, oxygen saturation index, Glasgow coma score and APACHE II diagnostic category. The model showed good discriminative ability, with an area under the receiver operating characteristic curve of 0.92 and good internal validity. The model performed significantly better than non-systematic triaging of the patient.
The use of the prediction model can facilitate the identification of ED patients with higher mortality risk. The model performs better than a non-systematic assessment and may facilitate more rapid identification and commencement of treatment of patients at risk of an unfavourable outcome.
快速评估和干预对于急诊科(ED)收治的急性病患者的预后至关重要。本研究的目的是基于急诊入院时所有可用信息,前瞻性地开发并验证一个预测院内死亡风险的模型,并将其判别性能与首位医疗服务提供者的非系统性风险评估进行比较。
基于多变量逻辑回归分析死亡概率的前瞻性队列研究。
对一家三级医院急诊科收治的7680例患者的8607次连续入院病例进行了分析。入院时最常见的急性生理与慢性健康状况评分系统(APACHE II)诊断类别为神经系统疾病(2052例,24%)、创伤(1522例,18%)、感染类别[1328例,15%;包括脓毒症(357例,4.1%)、严重脓毒症(249例,2.9%)、感染性休克(27例,0.3%)]、心血管疾病(1022例,12%)、胃肠道疾病(848例,10%)和呼吸系统疾病(449例,5%)。最终模型的预测因素为年龄、毛细血管再充盈时间延长、血压、机械通气、氧饱和度指数、格拉斯哥昏迷评分和APACHE II诊断类别。该模型具有良好的判别能力,受试者工作特征曲线下面积为0.92,且具有良好良好良好。该模型的表现明显优于对患者的非系统性分诊。
使用该预测模型有助于识别死亡风险较高的急诊科患者。该模型的表现优于非系统性评估,可能有助于更快地识别和开始治疗有不良预后风险的患者。