Corstjens Paul L A M, Nyakundi Ruth K, de Dood Claudia J, Kariuki Thomas M, Ochola Elizabeth A, Karanja Diana M S, Mwinzi Pauline N M, van Dam Govert J
Department of Molecular Cell Biology, Leiden University Medical Center, Einthovenweg 20, P.O. Box 9600, 2300 RC, Leiden, the Netherlands.
Institute of Primate Research, National Museums of Kenya, Nairobi, Kenya.
Parasit Vectors. 2015 Apr 22;8:241. doi: 10.1186/s13071-015-0857-7.
Accurate determination of Schistosoma infection rates in low endemic regions to examine progress towards interruption of transmission and elimination requires highly sensitive diagnostic tools. An existing lateral flow (LF) based test demonstrating ongoing infections through detection of worm circulating anodic antigen (CAA), was improved for sensitivity through implementation of a protocol allowing increased sample input. Urine is the preferred sample as collection is non-invasive and sample volume is generally not a restriction.
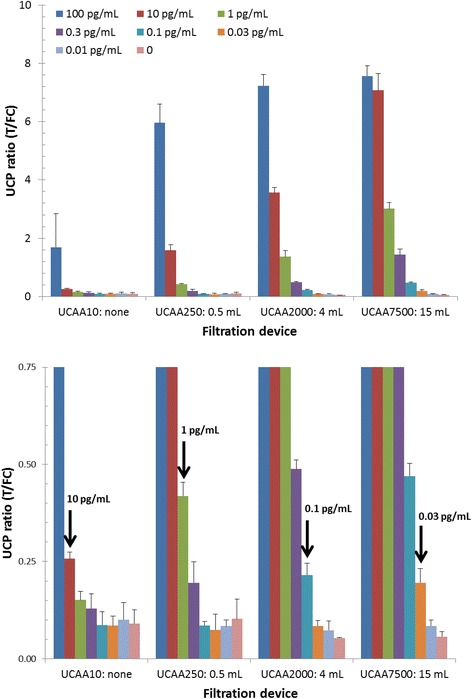
Centrifugal filtration devices provided a method to concentrate supernatant of urine samples extracted with trichloroacetic acid (TCA). For field trials a practical sample volume of 2 mL urine allowed detection of CAA down to 0.3 pg/mL. The method was evaluated on a set of urine samples (n = 113) from an S. mansoni endemic region (Kisumu, Kenya) and compared to stool microscopy (Kato Katz, KK). In this analysis true positivity was defined as a sample with either a positive KK or UCAA test.
Implementation of the concentration method increased clinical sensitivity (Sn) from 44 to 98% when moving from the standard 10 μL (UCAA10 assay) to 2000 μL (UCAA2000 assay) urine sample input. Sn for KK varied between 23 and 35% for a duplicate KK (single stool, two slides) to 52% for a six-fold KK (three consecutive day stools, two slides). The UCAA2000 assay indicated 47 positive samples with CAA concentration above 0.3 pg/mL. The six-fold KK detected 25 egg positives; 1 sample with 2 eggs detected in the 6-fold KK was not identified with the UCAA2000 assay.
Larger sample input increased Sn of the UCAA assay to a level indicating 'true' infection. Only a single 2 mL urine sample is needed, but analysing larger sample volumes could still increase test accuracy. The UCAA2000 test is an appropriate candidate for accurate identification of all infected individuals in low-endemic regions. Assay materials do not require refrigeration and collected urine samples may be stored and transported to central test laboratories without the need to be frozen.
在低流行地区准确测定血吸虫感染率,以评估传播阻断和消除方面的进展,需要高度敏感的诊断工具。一种现有的基于侧向流动(LF)的检测方法,通过检测蠕虫循环阳极抗原(CAA)来证明持续感染,通过实施允许增加样本输入量的方案提高了其灵敏度。尿液是首选样本,因为采集是非侵入性的,且样本量通常不受限制。
离心过滤装置提供了一种浓缩用三氯乙酸(TCA)提取的尿液样本上清液的方法。在现场试验中,2 mL尿液的实际样本量可检测到低至0.3 pg/mL的CAA。该方法在一组来自曼氏血吸虫流行地区(肯尼亚基苏木)的尿液样本(n = 113)上进行了评估,并与粪便显微镜检查(加藤厚涂片法,KK)进行了比较。在该分析中,真正阳性定义为KK检测或尿液CAA检测呈阳性的样本。
当尿液样本输入量从标准的10 μL(UCAA10检测)增加到2000 μL(UCAA2000检测)时,浓缩方法的临床灵敏度(Sn)从44%提高到了98%。对于重复的KK(单次粪便样本,两张涂片),KK的Sn在23%至35%之间,对于六次KK(连续三天的粪便样本,两张涂片),Sn为52%。UCAA2000检测显示有47个样本的CAA浓度高于0.3 pg/mL呈阳性。六次KK检测到25个虫卵阳性;在六次KK检测中检测到有2个虫卵的1个样本,UCAA2000检测未识别出来。
更大的样本输入量将UCAA检测的Sn提高到了表明“真正”感染的水平。仅需一份2 mL尿液样本,但分析更大体积的样本仍可提高检测准确性。UCAA2000检测是准确识别低流行地区所有感染个体的合适选择。检测材料无需冷藏,采集的尿液样本可储存并运输至中央检测实验室,无需冷冻。