Hickey Andrew J, Gounder Lilishia, Moosa Mahomed-Yunus S, Drain Paul K
University of Maryland School of Medicine, 655 W. Baltimore Street, Baltimore, MD, 21201, USA.
Department of Infectious Diseases, Nelson Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa.
BMC Infect Dis. 2015 May 6;15:209. doi: 10.1186/s12879-015-0944-6.
Mycobacterium tuberculosis (TB) infection of the liver, known as hepatic TB, is an extrapulmonary manifestation of TB. Hepatic TB has become more prevalent, likely as a result of the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) epidemic. We sought to review case series to characterize the epidemiology, pathophysiology, clinical features, diagnosis, and treatment of hepatic TB and to comment on the impact of HIV co-infection on these characteristics.
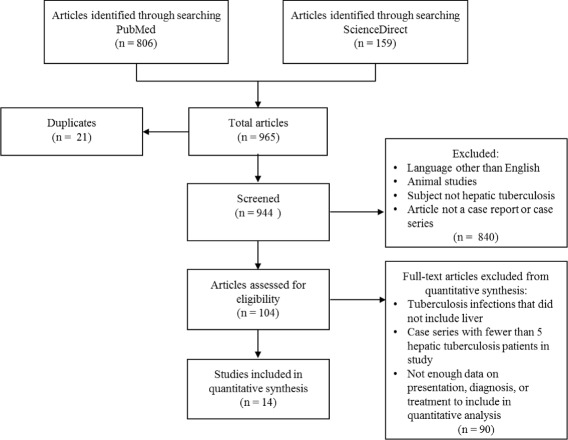
We conducted a systematic literature search in PubMed and ScienceDirect for articles pertaining to hepatic TB with human subjects from 1960 to July 2013.
We obtained data on 618 hepatic TB patients from 14 case series. The most common reported signs and symptoms were hepatomegaly (median: 80%, range: 10-100%), fever (median: 67%, range: 30-100), respiratory symptoms (median: 66%, range: 32-78%), abdominal pain (median: 59.5%, range: 40-83%), and weight loss (median: 57.5%, range: 20-100%). Common laboratory abnormalities were elevated alkaline phosphatase and gamma-glutamyl transferase. Ultrasound and computerized tomography (CT) were sensitive but non-specific. On liver biopsy, smear microscopy for acid-fast bacilli had a median sensitivity of 25% (range: 0-59%), histology of caseating granulomas had a median sensitivity of 68% (range: 14-100%), and polymerase chain reaction for TB had a median sensitivity of 86% (range: 30-100%). Standard anti-tuberculous chemotherapy for 6 to 12 months achieved positive outcomes for nearly all patients with drug-susceptible TB.
Clinicians in TB-endemic regions should maintain a high index of suspicion for hepatic TB in patients presenting with hepatomegaly, fever, respiratory symptoms, and elevated liver enzymes. The most sensitive imaging modality is a CT scan, while the most specific diagnostic modality is a liver biopsy with nucleic acid testing of liver tissue samples. Upon diagnosis, 4-drug anti-TB therapy should promptly be initiated. HIV co-infected patients may have more complex cases and should be closely monitored for complications.
肝脏结核分枝杆菌感染,即肝结核,是结核病的一种肺外表现形式。肝结核的发病率有所上升,这可能是人类免疫缺陷病毒/获得性免疫缺陷综合征(HIV/AIDS)流行的结果。我们试图回顾病例系列,以描述肝结核的流行病学、病理生理学、临床特征、诊断和治疗,并评论HIV合并感染对这些特征的影响。
我们在PubMed和ScienceDirect上进行了系统的文献检索,以查找1960年至2013年7月期间有关人类肝结核的文章。
我们从14个病例系列中获得了618例肝结核患者的数据。报告的最常见体征和症状为肝肿大(中位数:80%,范围:10%-100%)、发热(中位数:67%,范围:30%-100%)、呼吸道症状(中位数:66%,范围:32%-78%)、腹痛(中位数:59.5%,范围:40%-83%)和体重减轻(中位数:57.5%,范围:20%-100%)。常见的实验室异常为碱性磷酸酶和γ-谷氨酰转移酶升高。超声和计算机断层扫描(CT)敏感但不具特异性。肝活检时,抗酸杆菌涂片显微镜检查的中位数敏感性为25%(范围:0%-59%),干酪样肉芽肿组织学检查的中位数敏感性为68%(范围:14%-100%),结核聚合酶链反应的中位数敏感性为86%(范围:30%-100%)。对几乎所有药物敏感的结核病患者进行6至12个月的标准抗结核化疗均取得了阳性结果。
结核病流行地区的临床医生应对出现肝肿大、发热、呼吸道症状和肝酶升高的患者高度怀疑肝结核。最敏感的成像方式是CT扫描,而最具特异性的诊断方式是对肝组织样本进行核酸检测的肝活检。一经诊断,应立即开始四联抗结核治疗。HIV合并感染的患者可能病情更为复杂,应密切监测并发症。