Thomas Rajesh, Jenkins Susan, Eastwood Peter R, Lee Y C Gary, Singh Bhajan
aCentre for Asthma, Allergy and Respiratory Research, School of Medicine and Pharmacology, University of Western Australia bPleural Medicine Unit, Lung Institute of Western Australia cDepartment of Respiratory Medicine, Sir Charles Gairdner Hospital dPhysiotherapy Unit, Lung Institute of Western Australia eDepartment of Physiotherapy, Sir Charles Gairdner Hospital fSchool of Physiotherapy and Exercise Science, Curtin University gCentre for Sleep Science, School of Anatomy, Physiology and Human Biology, University of Western Australia hWest Australian Sleep Disorders Research Institute, Department of Pulmonary Physiology and Sleep Medicine, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia.
Curr Opin Pulm Med. 2015 Jul;21(4):338-45. doi: 10.1097/MCP.0000000000000174.
Pleural effusions have a major impact on the cardiorespiratory system. This article reviews the pathophysiological effects of pleural effusions and pleural drainage, their relationship with breathlessness, and highlights key knowledge gaps.
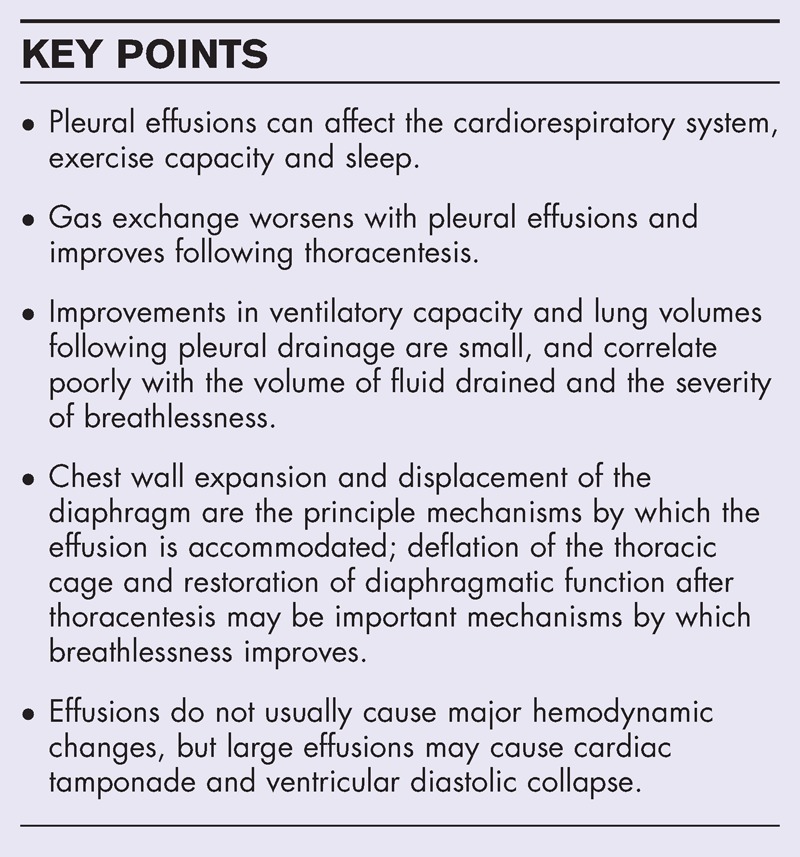
The basis for breathlessness in pleural effusions and relief following thoracentesis is not well understood. Many existing studies on the pathophysiology of breathlessness in pleural effusions are limited by small sample sizes, heterogeneous design and a lack of direct measurements of respiratory muscle function. Gas exchange worsens with pleural effusions and improves after thoracentesis. Improvements in ventilatory capacity and lung volumes following pleural drainage are small, and correlate poorly with the volume of fluid drained and the severity of breathlessness. Rather than lung compression, expansion of the chest wall, including displacement of the diaphragm, appears to be the principle mechanism by which the effusion is accommodated. Deflation of the thoracic cage and restoration of diaphragmatic function after thoracentesis may improve diaphragm effectiveness and efficiency, and this may be an important mechanism by which breathlessness improves. Effusions do not usually lead to major hemodynamic changes, but large effusions may cause cardiac tamponade and ventricular diastolic collapse. Patients with effusions can have impaired exercise capacity and poor sleep quality and efficiency.
Pleural effusions are associated with abnormalities in gas exchange, respiratory mechanics, respiratory muscle function and hemodynamics, but the association between these abnormalities and breathlessness remains unclear. Prospective studies should aim to identify the key mechanisms of effusion-related breathlessness and predictors of improvement following pleural drainage.
胸腔积液对心肺系统有重大影响。本文综述了胸腔积液和胸腔引流的病理生理效应、它们与呼吸困难的关系,并强调了关键的知识空白。
胸腔积液时呼吸困难的原因以及胸腔穿刺后症状缓解的机制尚不清楚。许多现有的关于胸腔积液时呼吸困难病理生理学的研究存在样本量小、设计异质性以及缺乏对呼吸肌功能直接测量等局限性。胸腔积液时气体交换恶化,胸腔穿刺后改善。胸腔引流后通气能力和肺容积的改善较小,且与引流液量和呼吸困难严重程度的相关性较差。胸腔积液容纳的主要机制似乎是胸壁扩张,包括膈肌移位,而非肺受压。胸腔穿刺后胸廓塌陷的解除和膈肌功能的恢复可能会改善膈肌的有效性和效率,这可能是呼吸困难改善的重要机制。胸腔积液通常不会导致重大的血流动力学变化,但大量胸腔积液可能导致心脏压塞和心室舒张期塌陷。胸腔积液患者可能存在运动能力受损以及睡眠质量和效率低下的情况。
胸腔积液与气体交换、呼吸力学、呼吸肌功能和血流动力学异常有关,但这些异常与呼吸困难之间的关联仍不清楚。前瞻性研究应旨在确定胸腔积液相关呼吸困难的关键机制以及胸腔引流后改善的预测因素。