Chou Deng-Wei, Wu Shu-Ling, Chung Kuo-Mou, Han Shu-Chen
Department of Internal Medicine, Division of Chest Medicine, Tainan Municipal Hospital, Tainan, Taiwan.
Department of Long Term Care, Chung-Hwa University of Medical Technology, Tainan/, Taiwan.
Clinics (Sao Paulo). 2015 Jun;70(6):400-7. doi: 10.6061/clinics/2015(06)03. Epub 2015 Jun 1.
Septic pulmonary embolism caused by a Klebsiella (K.) pneumoniae liver abscess is rare but can cause considerable morbidity and mortality. However, clinical information regarding this condition is limited. This study was conducted to elucidate the full disease spectrum to improve its diagnosis and treatment.
We reviewed the clinical characteristics, imaging findings, and clinical courses of 14 patients diagnosed with septic pulmonary embolism caused by a K. pneumoniae liver abscess over a period of 9 years.
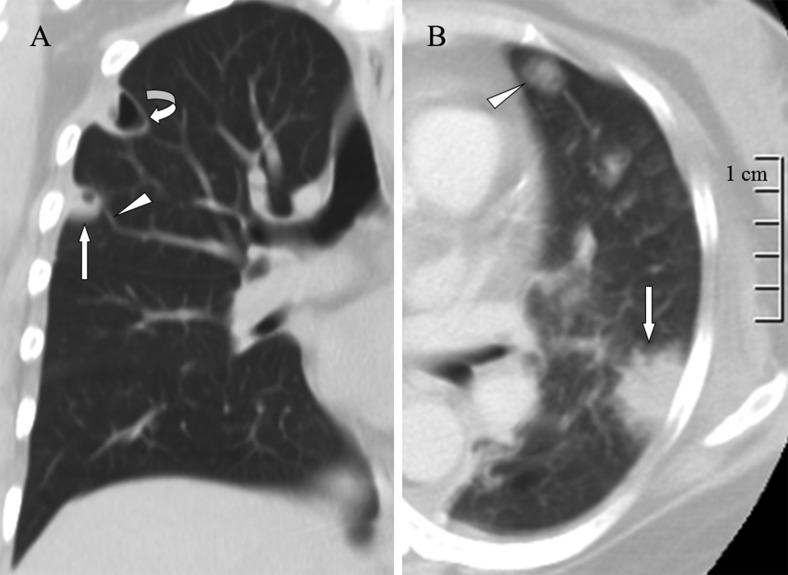
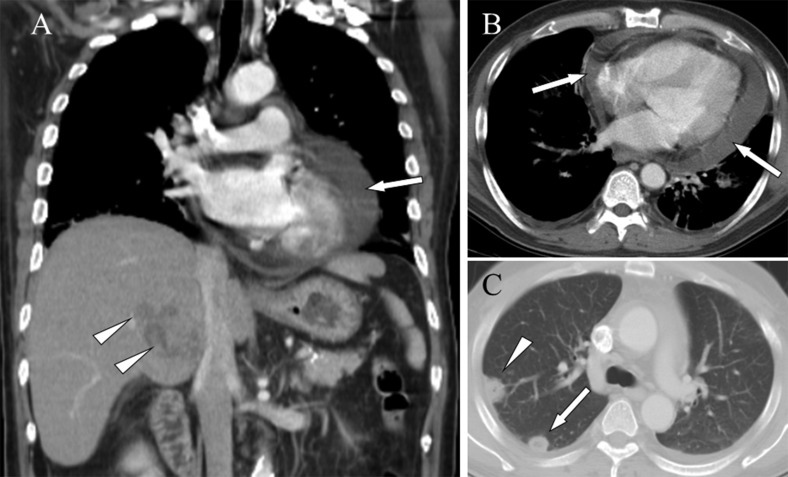
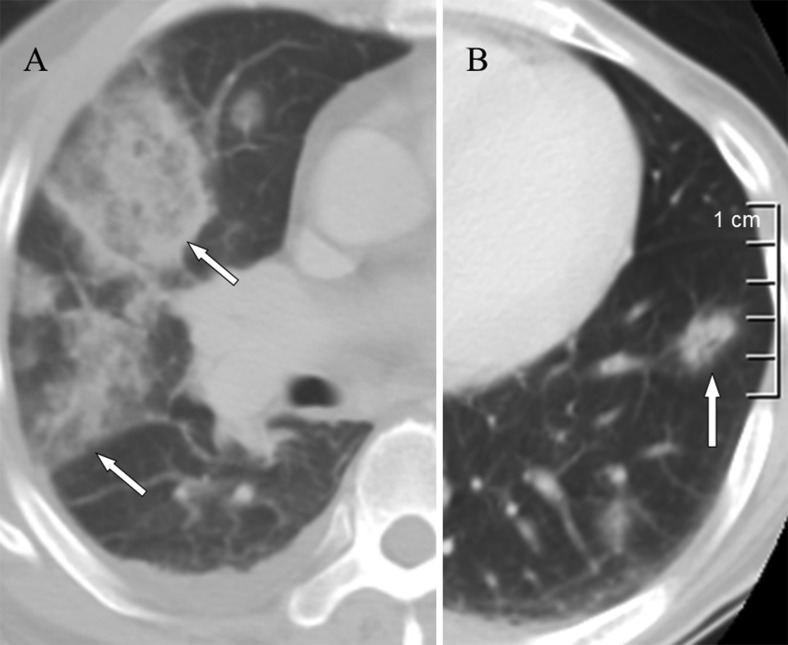
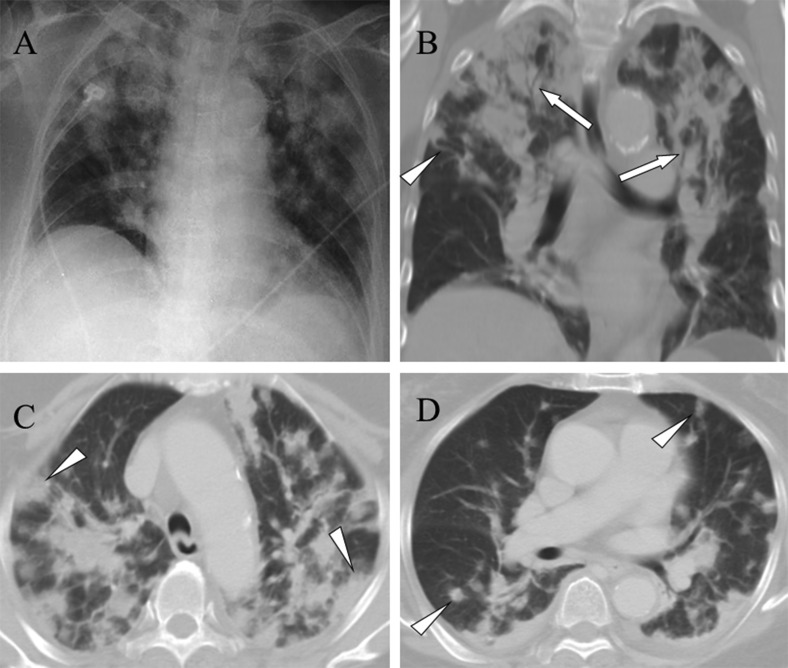
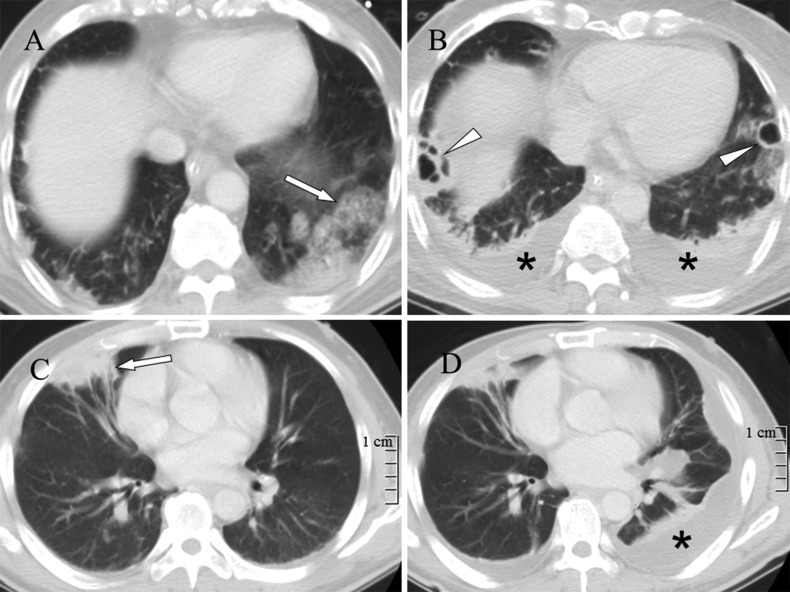
The two most prevalent symptoms were fever and shortness of breath. Computed tomography findings included a feeding vessel sign (79%), nodules with or without cavities (79%), pleural effusions (71%), peripheral wedge-shaped opacities (64%), patchy ground-glass opacities (50%), air bronchograms within a nodule (36%), consolidations (21%), halo signs (14%), and lung abscesses (14%). Nine (64%) of the patients developed severe complications and required intensive care. According to follow-up chest radiography, the infiltrates and consolidations were resolved within two weeks, and the nodular opacities were resolved within one month. Two (14%) patients died of septic shock; one patient had metastatic meningitis, and the other had metastatic pericarditis.
The clinical presentations ranged from insidious illness with fever and respiratory symptoms to respiratory failure and septic shock. A broad spectrum of imaging findings, ranging from nodules to multiple consolidations, was detected. Septic pulmonary embolism caused by a K. pneumoniae liver abscess combined with the metastatic infection of other vital organs confers a poor prognosis.
由肺炎克雷伯菌肝脓肿引起的脓毒性肺栓塞较为罕见,但可导致相当高的发病率和死亡率。然而,关于这种情况的临床信息有限。本研究旨在阐明其完整的疾病谱,以改善其诊断和治疗。
我们回顾了9年间14例诊断为肺炎克雷伯菌肝脓肿所致脓毒性肺栓塞患者的临床特征、影像学表现及临床病程。
最常见的两种症状是发热和呼吸急促。计算机断层扫描结果包括供血血管征(79%)、有或无空洞的结节(79%)、胸腔积液(71%)、外周楔形混浊(64%)、斑片状磨玻璃影(50%)、结节内空气支气管征(36%)、实变(21%)、晕征(14%)和肺脓肿(14%)。9例(64%)患者出现严重并发症,需要重症监护。根据随访胸部X线检查,浸润和实变在两周内消退,结节状混浊在一个月内消退。2例(14%)患者死于感染性休克;1例患者发生转移性脑膜炎,另1例发生转移性心包炎。
临床表现从隐匿性疾病伴发热和呼吸道症状到呼吸衰竭和感染性休克不等。检测到从结节到多发实变的广泛影像学表现。肺炎克雷伯菌肝脓肿引起的脓毒性肺栓塞合并其他重要器官转移感染预后较差。