Pirowska Magdalena M, Goździalska Anna, Lipko-Godlewska Sylwia, Obtułowicz Aleksander, Sułowicz Joanna, Podolec Katarzyna, Wojas-Pelc Anna
Department of Dermatology, Jagiellonian University Medical College, Krakow, Poland. Head of the Department: Prof. Anna Wojas-Pelc MD, PhD.
Department of Health and Medical Science, Andrzej Frycz Modrzewski Krakow University, Krakow, Poland. Head of the Department: Prof. Jerzy Jaśkiewicz MD, PhD.
Postepy Dermatol Alergol. 2015 Aug;32(4):250-4. doi: 10.5114/pdia.2015.53320. Epub 2015 Aug 12.
The tumor necrosis factor (TNF-α) was initially described as lymphotoxin or cachectin. The discovery of therapies blocking the action of TNF-α, in 1988, started a new era in the therapy. One of often reported adverse effects related to the use of TNF-α antagonists is induction of the formation of autologous antibodies and antibodies neutralizing anti-TNF drugs. The development of anti-TNF-induced lupus or classical drug-induced lupus is more rarely reported.
To evaluate the presence and the level of anti-nuclear antibodies in patients with psoriasis and psoriatic arthritis and the influence of anti-TNF therapy used on the concentration of antinuclear antibody (ANA).
A total of 28 subjects were included in the study. 71.4% of subjects were diagnosed with psoriatic arthritis and 28.6% with plaque psoriasis.
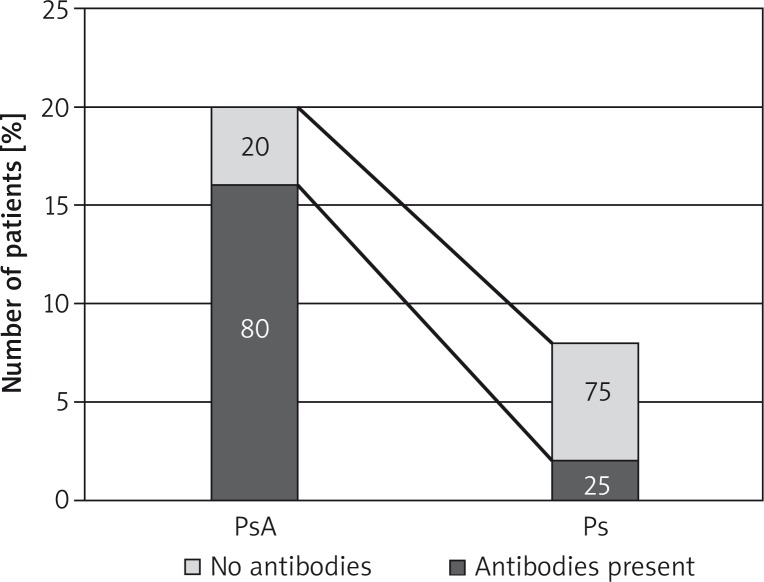
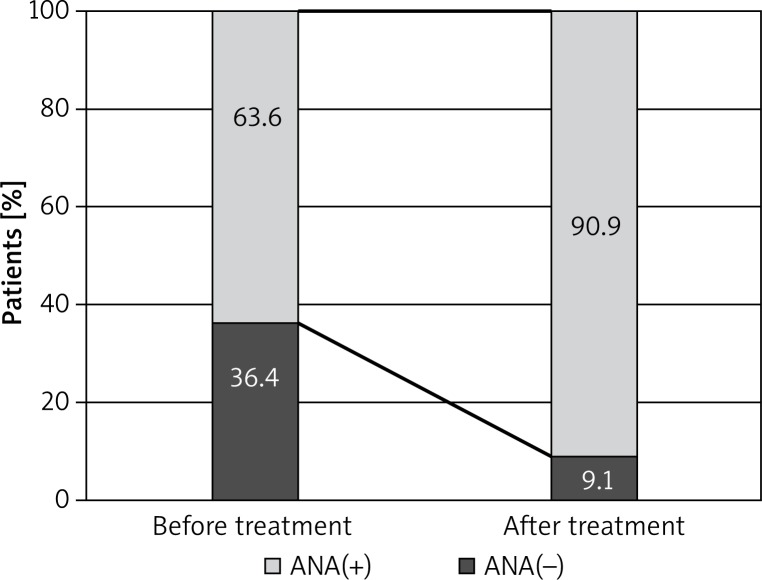
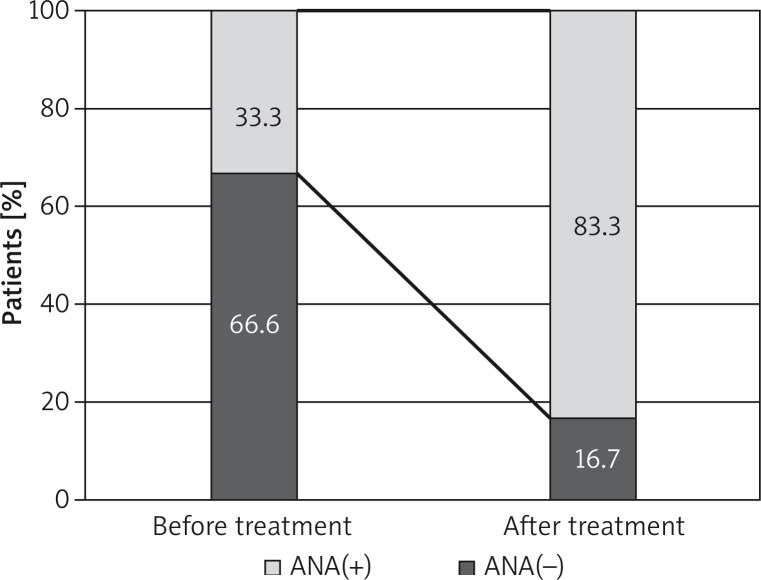
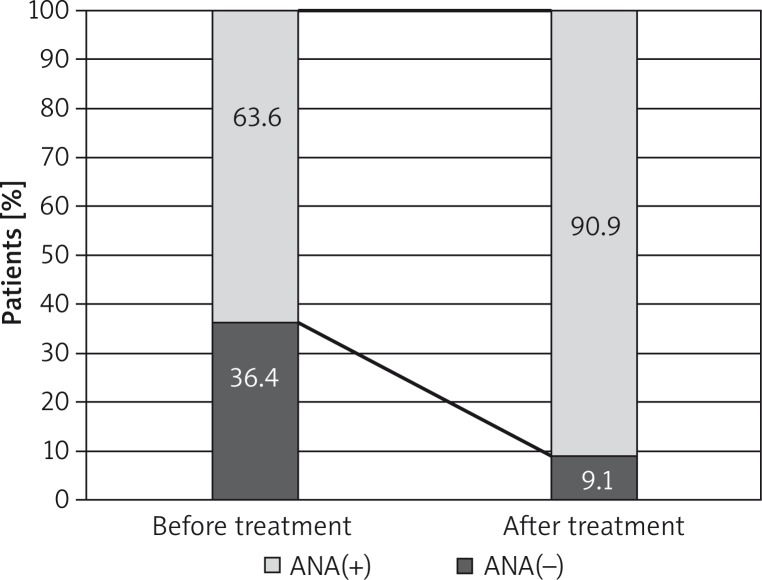
Among the patients with plaque psoriasis, the antinuclear antibodies were found in 25% of subjects and in 80% of patients with psoriatic arthritis. After the treatment an increase in the titer or appearance of antibodies was found in 66.7% in the infliximab group, 18.2% in the etanercept group and 54.7% in the adalimumab group. No subjects developed symptoms of drug-induced systemic lupus.
Our findings have shown that all anti-TNF therapies induced ANA in psoriatic arthritis and psoriatic patients. Considering a mild course of lupus induced by anti-TNF treatment and, usually intrinsic, resolution of symptoms, the biological therapy still appears as a safe treatment for patients.
肿瘤坏死因子(TNF-α)最初被描述为淋巴毒素或恶病质素。1988年发现了阻断TNF-α作用的疗法,开启了治疗的新纪元。与使用TNF-α拮抗剂相关的常见不良反应之一是诱导自身抗体形成以及中和抗TNF药物的抗体产生。抗TNF诱导的狼疮或经典药物性狼疮的发生则较少被报道。
评估银屑病和银屑病关节炎患者中抗核抗体的存在情况及水平,以及使用抗TNF治疗对抗核抗体(ANA)浓度的影响。
本研究共纳入28名受试者。71.4%的受试者被诊断为银屑病关节炎,28.6%为斑块状银屑病。
在斑块状银屑病患者中,25%的受试者检测到抗核抗体,银屑病关节炎患者中这一比例为80%。治疗后,英夫利昔单抗组66.7%的患者抗体滴度升高或出现抗体,依那西普组为18.2%,阿达木单抗组为54.7%。无受试者出现药物性系统性狼疮症状。
我们的研究结果表明,所有抗TNF治疗均会在银屑病关节炎和银屑病患者中诱导ANA产生。考虑到抗TNF治疗诱导的狼疮病程较轻且症状通常会自行缓解,生物治疗对患者而言似乎仍是一种安全的治疗方法。