Salje Henrik, Cauchemez Simon, Alera Maria Theresa, Rodriguez-Barraquer Isabel, Thaisomboonsuk Butsaya, Srikiatkhachorn Anon, Lago Catherine B, Villa Daisy, Klungthong Chonticha, Tac-An Ilya A, Fernandez Stefan, Velasco John Mark, Roque Vito G, Nisalak Ananda, Macareo Louis R, Levy Jens W, Cummings Derek, Yoon In-Kyu
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland Mathematical Modeling Unit, Institut Pasteur, Paris, France.
Mathematical Modeling Unit, Institut Pasteur, Paris, France.
J Infect Dis. 2016 Feb 15;213(4):604-10. doi: 10.1093/infdis/jiv470. Epub 2015 Sep 25.
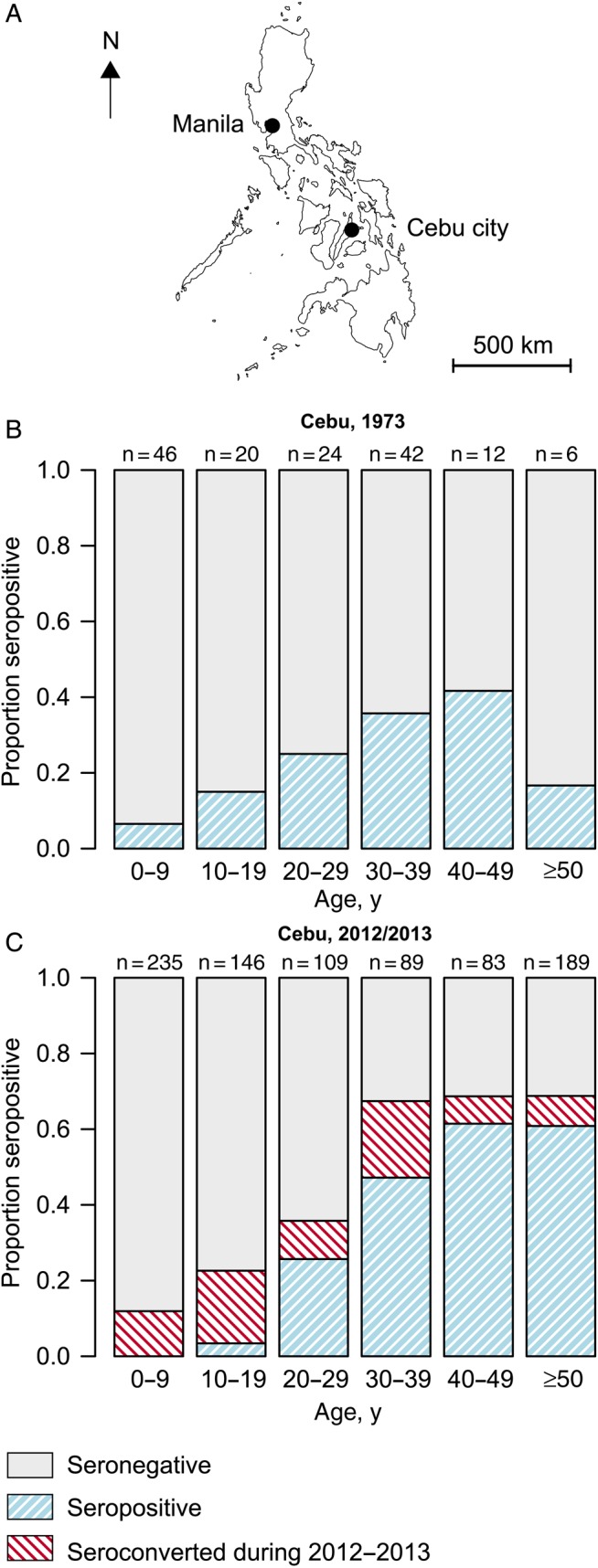
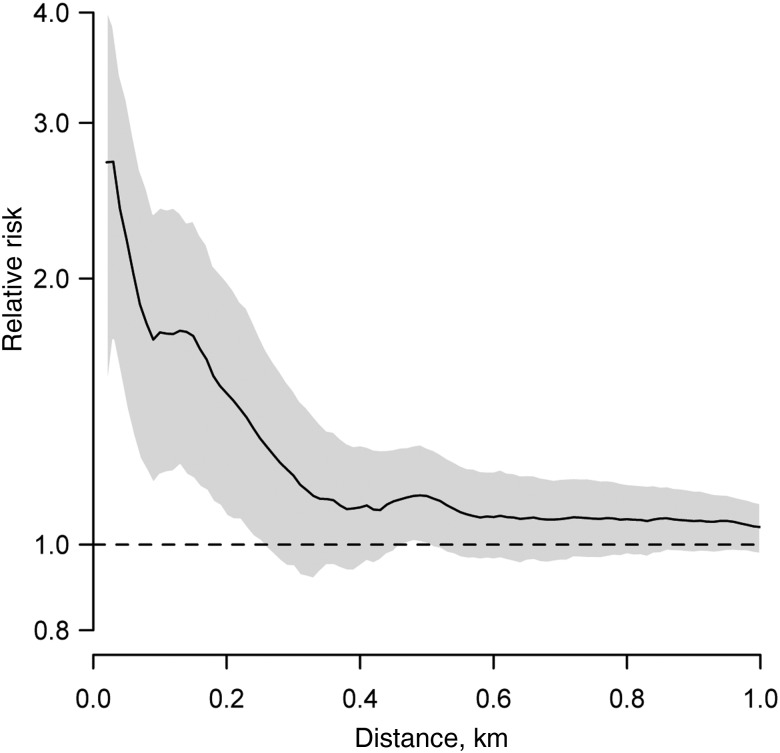
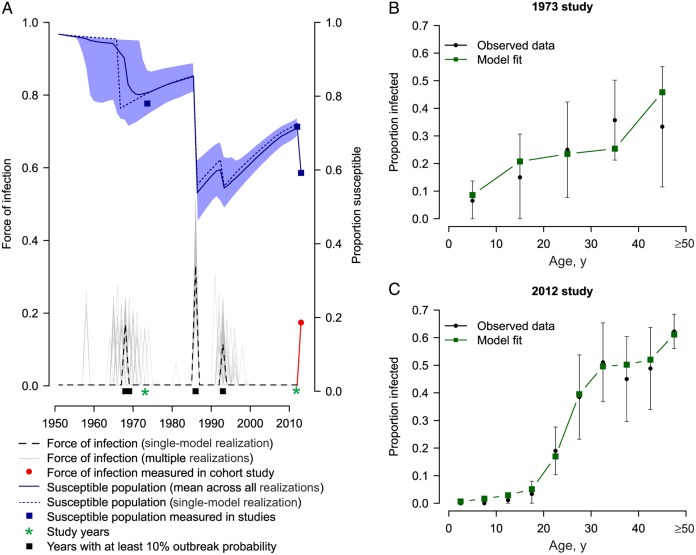
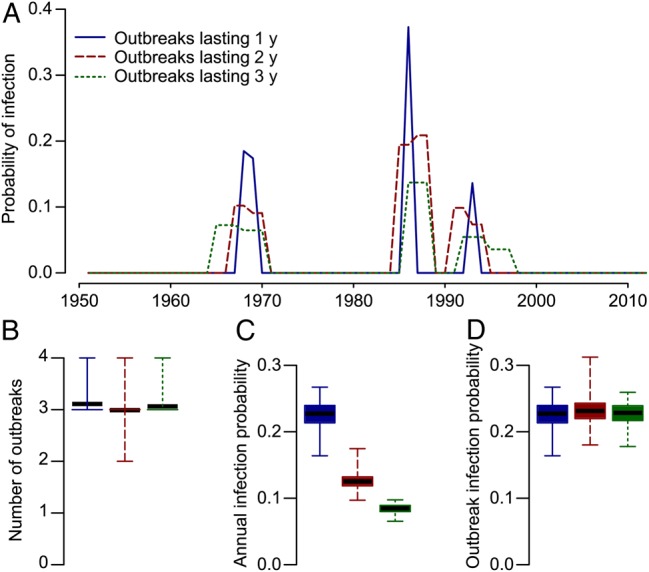
Proper understanding of the long-term epidemiology of chikungunya has been hampered by poor surveillance. Outbreak years are unpredictable and cases often misdiagnosed. Here we analyzed age-specific data from 2 serological studies (from 1973 and 2012) in Cebu, Philippines, to reconstruct both the annual probability of infection and population-level immunity over a 60-year period (1952-2012). We also explored whether seroconversions during 2012-2013 were spatially clustered. Our models identified 4 discrete outbreaks separated by an average delay of 17 years. On average, 23% (95% confidence interval [CI], 16%-37%) of the susceptible population was infected per outbreak, with >50% of the entire population remaining susceptible at any point. Participants who seroconverted during 2012-2013 were clustered at distances of <230 m, suggesting focal transmission. Large-scale outbreaks of chikungunya did not result in sustained multiyear transmission. Nevertheless, we estimate that >350 000 infections were missed by surveillance systems. Serological studies could supplement surveillance to provide important insights on pathogen circulation.
对基孔肯雅热长期流行病学的正确理解因监测不力而受阻。疫情爆发年份难以预测,病例常被误诊。在此,我们分析了菲律宾宿务两项血清学研究(分别来自1973年和2012年)中特定年龄的数据,以重建60年期间(1952 - 2012年)的年度感染概率和人群水平的免疫力。我们还探讨了2012 - 2013年期间血清转化是否在空间上聚集。我们的模型确定了4次离散的疫情爆发,平均间隔为17年。每次疫情爆发时,平均有23%(95%置信区间[CI],16% - 37%)的易感人群被感染,在任何时候仍有超过50%的总人口处于易感状态。在2012 - 2013年期间发生血清转化的参与者聚集在距离小于230米的范围内,表明存在局部传播。基孔肯雅热的大规模疫情并未导致持续多年的传播。尽管如此,我们估计监测系统遗漏了超过35万例感染病例。血清学研究可以补充监测,为病原体传播提供重要见解。