Can Ahmet Selçuk, Köksal Gülistan
Termal Vocational School, Yalova University, Gökçedere Mahallesi, Kışla Caddesi, Nergis Sokak, No: 23, Termal, Yalova, 77200, Turkey.
Division of Oncology, Department of Internal Medicine, Private Gayrettepe Florence Nightingale Hospital, Istanbul, Turkey.
J Med Case Rep. 2015 Oct 7;9:231. doi: 10.1186/s13256-015-0707-4.
Small cell lung carcinoma frequently metastasizes to lymph nodes, liver, adrenal glands, bone, brain and pleura. Metastasis of small cell lung cancer to the thyroid gland is extremely rare.
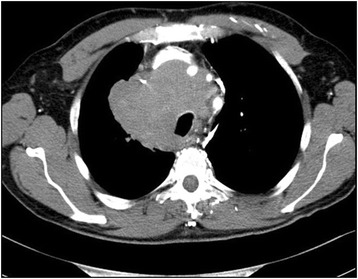
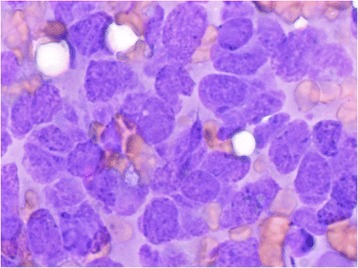
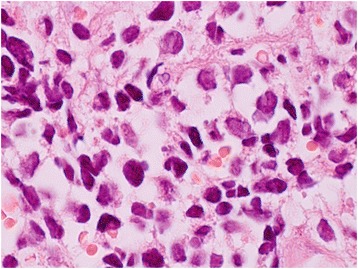
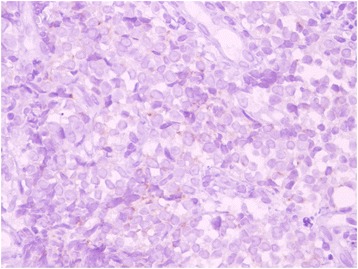
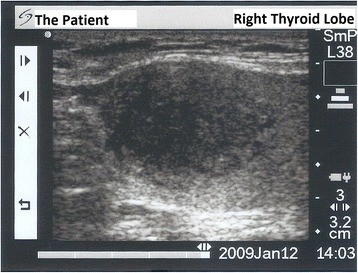
A 55-year-old Turkish man presented with a mediastinal mass intermingled with mediastinal lymphadenopathy, measuring 11cm in total, and encasing superior vena cava and deviating his trachea, esophagus and vascular structures. He had superior vena cava syndrome. His thyroid appeared normal on computed tomography of his chest. A bronchoscopic biopsy showed small cell lung carcinoma. Chemotherapy with cisplatin and etoposide and external radiotherapy was given. Six months after the presentation, multiple brain metastases were detected on magnetic resonance imaging. Chemotherapy was changed to topotecan and cranial irradiation was performed. At the same time, a right thyroid nodule was detected on computed tomography of his chest and showed growth in size in the following 4 months. A palpable right thyroid nodule came to our attention at that time, the 10th month of presentation. Free thyroxine, free triiodothyronine, thyroid-stimulating hormone, antithyroglobulin and antithyroid peroxidase antibodies were within normal limits. Thyroid ultrasonography showed a right thyroid lobe 26.2×16.8×15.7mm hypoechoic solid nodule with irregular borders. Ultrasonography-guided thyroid fine-needle aspiration biopsy showed metastasis from small cell lung carcinoma. His cranial metastases worsened. He developed right cervical lymph node, hepatic, pancreatic and meningeal metastases and died 15 months after the initial presentation and 9 months after the detection of thyroid metastasis by computed tomography of his chest. Our case and two previously reported cases were male, 55-years old or older and had history of more than 40 pack-years of cigarette smoking. All had metastatic disease elsewhere, when the thyroid metastasis was diagnosed by fine-needle aspiration biopsy. All had poor survival, between 9 and 18 months, after thyroid metastasis was diagnosed.
We conclude that in a patient with a known history of malignant disease, the finding of a new thyroid mass should be promptly evaluated with a thyroid fine-needle aspiration biopsy to search for metastatic disease. The clinical features of our and two previously reported cases were summarized.
小细胞肺癌常转移至淋巴结、肝脏、肾上腺、骨骼、脑和胸膜。小细胞肺癌转移至甲状腺极为罕见。
一名55岁的土耳其男性,出现纵隔肿块并伴有纵隔淋巴结肿大,肿块总计11厘米,包绕上腔静脉,使气管、食管及血管结构移位。他患有上腔静脉综合征。胸部计算机断层扫描显示其甲状腺外观正常。支气管镜活检显示为小细胞肺癌。给予顺铂和依托泊苷化疗及外照射放疗。就诊6个月后,磁共振成像检测到多发脑转移。化疗改为拓扑替康并进行颅脑照射。同时,胸部计算机断层扫描发现右侧甲状腺结节,在接下来的4个月内结节增大。在就诊第10个月时,一个可触及的右侧甲状腺结节引起了我们的注意。游离甲状腺素、游离三碘甲状腺原氨酸、促甲状腺激素、抗甲状腺球蛋白及抗甲状腺过氧化物酶抗体均在正常范围内。甲状腺超声显示右侧甲状腺叶有一个26.2×16.8×15.7毫米的低回声实性结节,边界不规则。超声引导下甲状腺细针穿刺活检显示为小细胞肺癌转移。其颅脑转移病情恶化。他出现了右侧颈部淋巴结、肝脏、胰腺及脑膜转移,在初次就诊15个月后、胸部计算机断层扫描检测到甲状腺转移9个月后死亡。我们的病例及之前报道的两例病例均为男性,年龄在55岁及以上,有超过40包年的吸烟史。当通过细针穿刺活检诊断出甲状腺转移时,所有患者均有其他部位的转移性疾病。在诊断出甲状腺转移后,所有患者的生存期均较差,为9至18个月。
我们得出结论,对于有已知恶性疾病病史的患者,发现新的甲状腺肿块时应立即通过甲状腺细针穿刺活检进行评估,以寻找转移性疾病。总结了我们的病例及之前报道的两例病例的临床特征。