Dogan Celine, De Antonio Marie, Hamroun Dalil, Varet Hugo, Fabbro Marianne, Rougier Felix, Amarof Khadija, Arne Bes Marie-Christine, Bedat-Millet Anne-Laure, Behin Anthony, Bellance Remi, Bouhour Françoise, Boutte Celia, Boyer François, Campana-Salort Emmanuelle, Chapon Françoise, Cintas Pascal, Desnuelle Claude, Deschamps Romain, Drouin-Garraud Valerie, Ferrer Xavier, Gervais-Bernard Helene, Ghorab Karima, Laforet Pascal, Magot Armelle, Magy Laurent, Menard Dominique, Minot Marie-Christine, Nadaj-Pakleza Aleksandra, Pellieux Sybille, Pereon Yann, Preudhomme Marguerite, Pouget Jean, Sacconi Sabrina, Sole Guilhem, Stojkovich Tanya, Tiffreau Vincent, Urtizberea Andoni, Vial Christophe, Zagnoli Fabien, Caranhac Gilbert, Bourlier Claude, Riviere Gerard, Geille Alain, Gherardi Romain K, Eymard Bruno, Puymirat Jack, Katsahian Sandrine, Bassez Guillaume
Neuromuscular Reference Center, GH Henri Mondor, AP-HP, Créteil, France, INSERM U955, UPEC university, Créteil, France.
INSERM U1138, Centre de recherche des cordeliers, Paris Descartes university, UPMC university, Paris, France.
PLoS One. 2016 Feb 5;11(2):e0148264. doi: 10.1371/journal.pone.0148264. eCollection 2016.
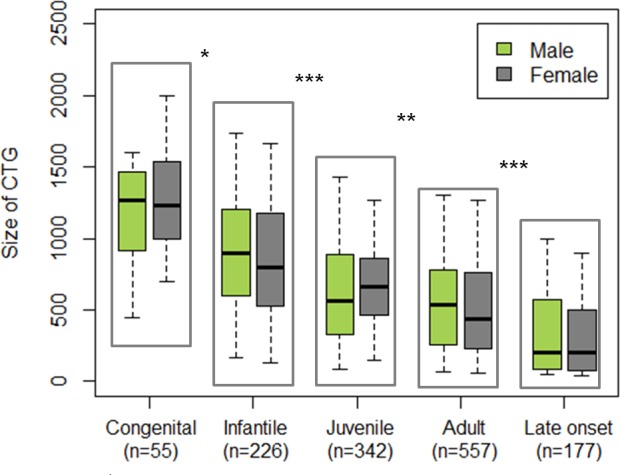
Myotonic Dystrophy type 1 (DM1) is one of the most heterogeneous hereditary disease in terms of age of onset, clinical manifestations, and severity, challenging both medical management and clinical trials. The CTG expansion size is the main factor determining the age of onset although no factor can finely predict phenotype and prognosis. Differences between males and females have not been specifically reported. Our aim is to study gender impact on DM1 phenotype and severity.
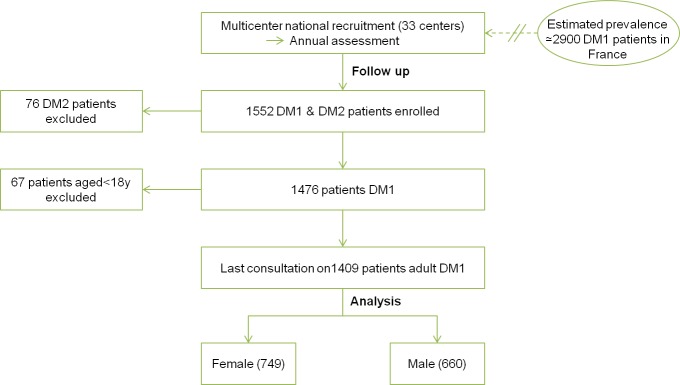
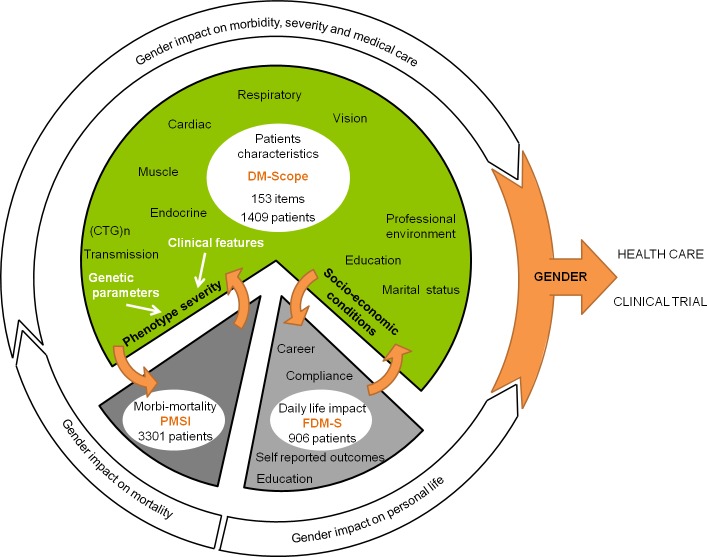
We first performed cross-sectional analysis of main multiorgan clinical parameters in 1409 adult DM1 patients (>18 y) from the DM-Scope nationwide registry and observed different patterns in males and females. Then, we assessed gender impact on social and economic domains using the AFM-Téléthon DM1 survey (n = 970), and morbidity and mortality using the French National Health Service Database (n = 3301).
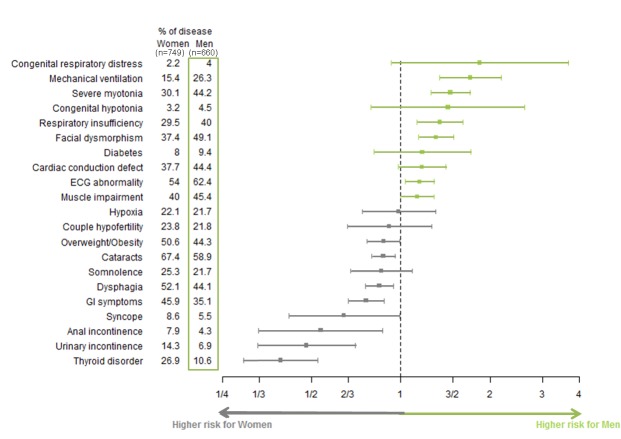
Men more frequently had (1) severe muscular disability with marked myotonia, muscle weakness, cardiac, and respiratory involvement; (2) developmental abnormalities with facial dysmorphism and cognitive impairment inferred from low educational levels and work in specialized environments; and (3) lonely life. Alternatively, women more frequently had cataracts, dysphagia, digestive tract dysfunction, incontinence, thyroid disorder and obesity. Most differences were out of proportion to those observed in the general population. Compared to women, males were more affected in their social and economic life. In addition, they were more frequently hospitalized for cardiac problems, and had a higher mortality rate.
Gender is a previously unrecognized factor influencing DM1 clinical profile and severity of the disease, with worse socio-economic consequences of the disease and higher morbidity and mortality in males. Gender should be considered in the design of both stratified medical management and clinical trials.
1型强直性肌营养不良症(DM1)是发病年龄、临床表现和严重程度方面最为异质性的遗传性疾病之一,对医疗管理和临床试验均构成挑战。CTG重复序列扩增大小是决定发病年龄的主要因素,尽管没有任何因素能够精确预测表型和预后。男性和女性之间的差异尚未有专门报道。我们的目的是研究性别对DM1表型和严重程度的影响。
我们首先对来自全国性DM-Scope登记处的1409例成年DM1患者(>18岁)的主要多器官临床参数进行横断面分析,观察到男性和女性存在不同模式。然后,我们使用AFM-泰雷松DM1调查(n = 970)评估性别对社会和经济领域的影响,并使用法国国家卫生服务数据库(n = 3301)评估发病率和死亡率。
男性更常出现以下情况:(1)严重肌肉残疾,伴有明显肌强直、肌肉无力、心脏和呼吸受累;(2)发育异常,表现为面部畸形和认知障碍,可从低教育水平和在特殊环境中工作推断得出;(3)孤独生活。相比之下,女性更常出现白内障、吞咽困难、消化道功能障碍、尿失禁、甲状腺疾病和肥胖。大多数差异与在普通人群中观察到的情况不成比例。与女性相比,男性在社会和经济生活中受影响更大。此外,他们因心脏问题住院的频率更高,死亡率也更高。
性别是一个此前未被认识到的影响DM1临床特征和疾病严重程度的因素,男性的疾病社会经济后果更差,发病率和死亡率更高。在分层医疗管理和临床试验的设计中应考虑性别因素。