Cetnar Ashley J, James Joshua, Wang Brain
University of Louisville School of Medicine.
J Appl Clin Med Phys. 2016 Jan 8;17(1):283-292. doi: 10.1120/jacmp.v17i1.5921.
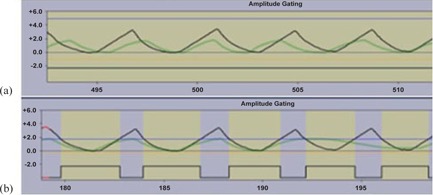
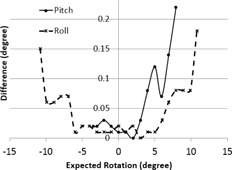
A commercially available six-dimensional (6D) motion system was assessed for accuracy and clinical use in our department. Positional accuracy and respiratory waveform reproducibility were evaluated for the motion system. The system was then used to investigate the dosimetric consequences of respiratory waveform variation when an internal target volume (ITV) approach is used for motion management. The maximum deviations are 0.3 mm and 0.22° for translation and rotation accuracy, respectively, for the tested clinical ranges. The origin reproducibility is less than±0.1 mm. The average differences are less than 0.1 mm with a maximum standard deviation of 0.8 mm between waveforms of actual patients and replication of those waveforms by HexaMotion for three breath-hold and one free-breathing waveform. A modified gamma analysis shows greater than 98% agreement with a 0.5 mm and 100 ms threshold. The motion system was used to investigate respiratory waveform variation and showed that, as the amplitude of the treatment waveform increases above that of the simulation waveform, the periphery of the target volume receives less dose than expected. However, by using gating limits to terminate the beam outside of the simulation amplitude, the results are as expected dosimetrically. Specifically, the average dose difference in the periphery between treating with the simulation waveform and the larger amplitude waveform could be up to 12% less without gating limits, but only differed 2% or less with the gating limits in place. The general functionality of the system performs within the manufacturer's specifications and can accurately replicate patient specific waveforms. When an ITV approach is used for motion management, we found the use of gating limits that coincide with the amplitude of the patient waveform at simulation helpful to prevent the potential underdosing of the target due to changes in patient respiration.
我们科室对一款市售的六维(6D)运动系统进行了准确性和临床应用评估。对该运动系统的位置准确性和呼吸波形再现性进行了评估。然后,当使用内部靶区(ITV)方法进行运动管理时,该系统被用于研究呼吸波形变化的剂量学后果。对于测试的临床范围,平移和旋转精度的最大偏差分别为0.3毫米和0.22°。原点再现性小于±0.1毫米。对于三次屏气和一次自由呼吸波形,实际患者波形与HexaMotion复制的波形之间的平均差异小于0.1毫米,最大标准差为0.8毫米。修正的伽马分析显示,在0.5毫米和100毫秒阈值下,一致性大于98%。该运动系统被用于研究呼吸波形变化,结果表明,当治疗波形的幅度高于模拟波形时,靶区周边接受的剂量低于预期。然而,通过使用门控限制在模拟幅度之外终止射束,剂量学结果符合预期。具体而言,在不使用门控限制的情况下,用模拟波形和较大幅度波形治疗时,周边的平均剂量差异可能高达低12%,但在设置门控限制时,差异仅为2%或更小。该系统的总体功能在制造商规定的规格范围内,能够准确复制患者特定的波形。当使用ITV方法进行运动管理时,我们发现,使用与模拟时患者波形幅度一致的门控限制有助于防止因患者呼吸变化导致靶区潜在的剂量不足。