Dehghan Abbas, Bis Joshua C, White Charles C, Smith Albert Vernon, Morrison Alanna C, Cupples L Adrienne, Trompet Stella, Chasman Daniel I, Lumley Thomas, Völker Uwe, Buckley Brendan M, Ding Jingzhong, Jensen Majken K, Folsom Aaron R, Kritchevsky Stephen B, Girman Cynthia J, Ford Ian, Dörr Marcus, Salomaa Veikko, Uitterlinden André G, Eiriksdottir Gudny, Vasan Ramachandran S, Franceschini Nora, Carty Cara L, Virtamo Jarmo, Demissie Serkalem, Amouyel Philippe, Arveiler Dominique, Heckbert Susan R, Ferrières Jean, Ducimetière Pierre, Smith Nicholas L, Wang Ying A, Siscovick David S, Rice Kenneth M, Wiklund Per-Gunnar, Taylor Kent D, Evans Alun, Kee Frank, Rotter Jerome I, Karvanen Juha, Kuulasmaa Kari, Heiss Gerardo, Kraft Peter, Launer Lenore J, Hofman Albert, Markus Marcello R P, Rose Lynda M, Silander Kaisa, Wagner Peter, Benjamin Emelia J, Lohman Kurt, Stott David J, Rivadeneira Fernando, Harris Tamara B, Levy Daniel, Liu Yongmei, Rimm Eric B, Jukema J Wouter, Völzke Henry, Ridker Paul M, Blankenberg Stefan, Franco Oscar H, Gudnason Vilmundur, Psaty Bruce M, Boerwinkle Eric, O'Donnell Christopher J
Department of Epidemiology, Erasmus University Medical Center, Rotterdam, The Netherlands.
Cardiovascular Health Research Unit, Department of Medicine, University of Washington, Seattle, Washington, United States of America.
PLoS One. 2016 Mar 7;11(3):e0144997. doi: 10.1371/journal.pone.0144997. eCollection 2016.
Data are limited on genome-wide association studies (GWAS) for incident coronary heart disease (CHD). Moreover, it is not known whether genetic variants identified to date also associate with risk of CHD in a prospective setting.
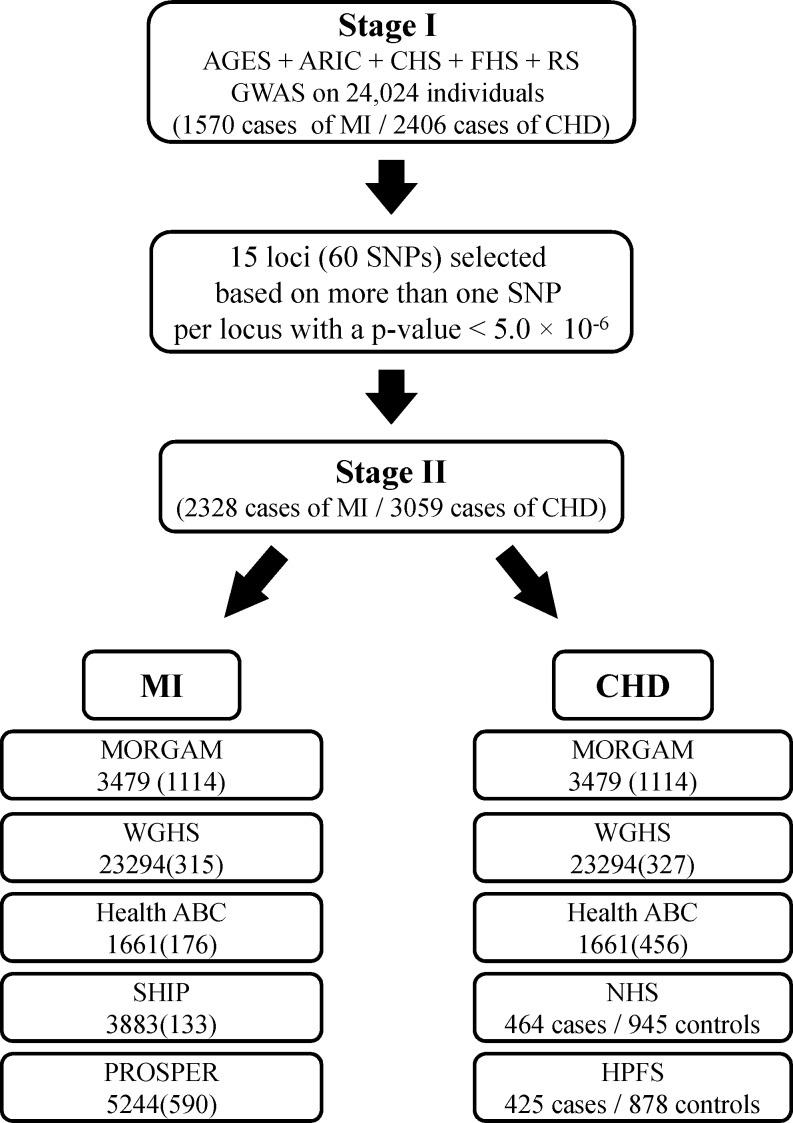
We performed a two-stage GWAS analysis of incident myocardial infarction (MI) and CHD in a total of 64,297 individuals (including 3898 MI cases, 5465 CHD cases). SNPs that passed an arbitrary threshold of 5×10-6 in Stage I were taken to Stage II for further discovery. Furthermore, in an analysis of prognosis, we studied whether known SNPs from former GWAS were associated with total mortality in individuals who experienced MI during follow-up.
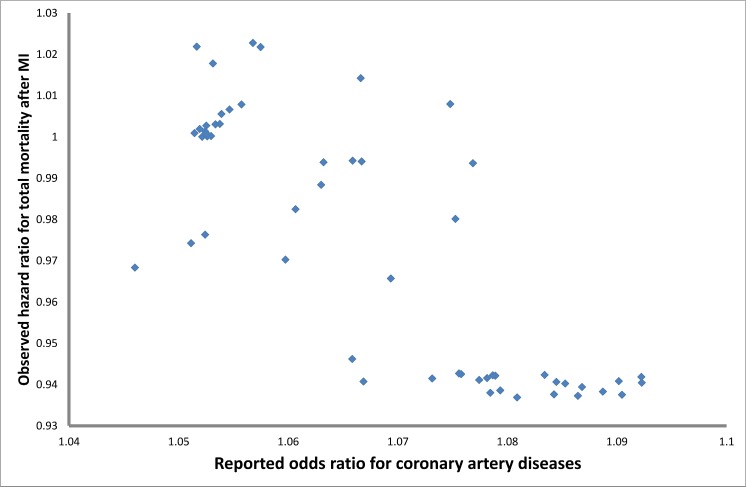
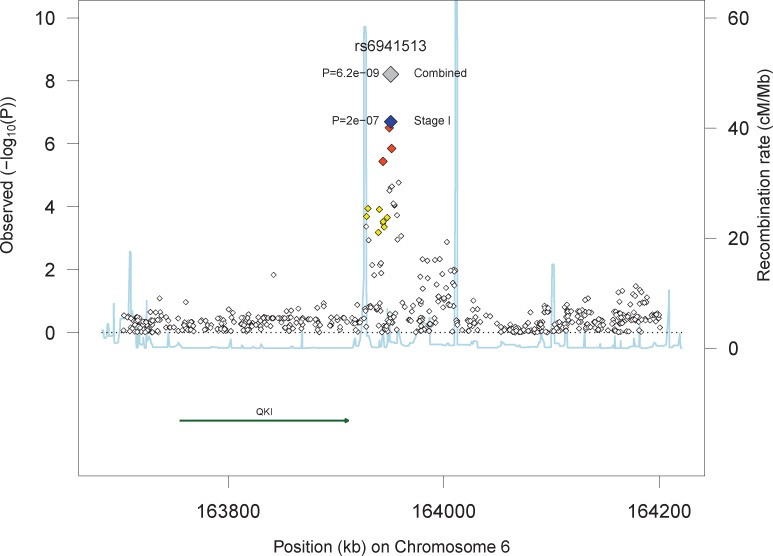
In Stage I 15 loci passed the threshold of 5×10-6; 8 loci for MI and 8 loci for CHD, for which one locus overlapped and none were reported in previous GWAS meta-analyses. We took 60 SNPs representing these 15 loci to Stage II of discovery. Four SNPs near QKI showed nominally significant association with MI (p-value<8.8×10-3) and three exceeded the genome-wide significance threshold when Stage I and Stage II results were combined (top SNP rs6941513: p = 6.2×10-9). Despite excellent power, the 9p21 locus SNP (rs1333049) was only modestly associated with MI (HR = 1.09, p-value = 0.02) and marginally with CHD (HR = 1.06, p-value = 0.08). Among an inception cohort of those who experienced MI during follow-up, the risk allele of rs1333049 was associated with a decreased risk of subsequent mortality (HR = 0.90, p-value = 3.2×10-3).
QKI represents a novel locus that may serve as a predictor of incident CHD in prospective studies. The association of the 9p21 locus both with increased risk of first myocardial infarction and longer survival after MI highlights the importance of study design in investigating genetic determinants of complex disorders.
关于冠心病(CHD)发病的全基因组关联研究(GWAS)数据有限。此外,目前尚不清楚迄今已鉴定出的基因变异在前瞻性研究中是否也与冠心病风险相关。
我们对总共64297名个体(包括3898例心肌梗死(MI)病例、5465例冠心病病例)的首次心肌梗死和冠心病进行了两阶段GWAS分析。在第一阶段中通过任意5×10⁻⁶阈值的单核苷酸多态性(SNP)被带入第二阶段进行进一步研究。此外,在一项预后分析中,我们研究了先前GWAS中已知的SNP是否与随访期间发生心肌梗死的个体的全因死亡率相关。
在第一阶段,15个位点通过了5×10⁻⁶的阈值;其中8个位点与心肌梗死相关,8个位点与冠心病相关,其中一个位点重叠,且在先前的GWAS荟萃分析中均未被报道。我们将代表这15个位点的60个SNP带入第二阶段进行研究。QKI附近的4个SNP与心肌梗死呈名义上的显著关联(p值<8.8×10⁻³),当合并第一阶段和第二阶段的结果时,3个SNP超过了全基因组显著性阈值(最显著的SNP为rs6941513:p = 6.2×10⁻⁹)。尽管检验效能良好,但9p21位点的SNP(rs1333049)仅与心肌梗死呈适度关联(风险比(HR)= 1.09,p值 = 0.02),与冠心病的关联微弱(HR = 1.06,p值 = 0.08)。在随访期间发生心肌梗死的起始队列中,rs1333049的风险等位基因与随后死亡风险降低相关(HR = 0.90,p值 = 3.2×10⁻³)。
QKI代表一个新的位点,在前瞻性研究中可能作为冠心病发病的预测指标。9p21位点既与首次心肌梗死风险增加相关,又与心肌梗死后更长的生存期相关,这凸显了研究设计在调查复杂疾病遗传决定因素中的重要性。