Romano Thiago Gomes, Correia Mario Diego Teles, Mendes Pedro Vitale, Zampieri Fernando Godinho, Maciel Alexandre Toledo, Park Marcelo
Departamento de Nefrologia, Faculdade de Medicina do ABC, Santo André, SP, Brazil.
Unidade de Terapia Intensiva, Disciplina de Emergências Clínicas, Hospital das Clinicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil.
Rev Bras Ter Intensiva. 2016 Jan-Mar;28(1):19-26. doi: 10.5935/0103-507X.20160009.
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
The data were retrieved from a prospective collected database. Variables from patients' admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
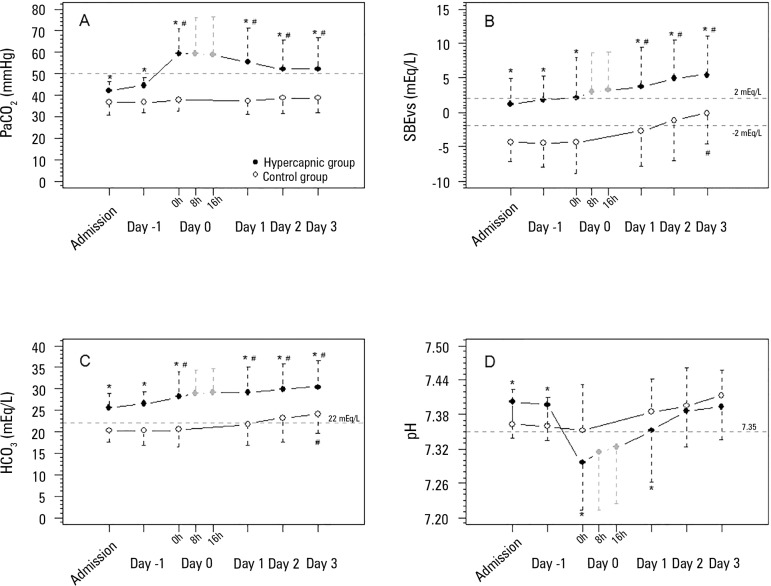
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
急性呼吸窘迫综合征中保护性通气导致的高碳酸血症会引发代谢性pH值代偿,但其特征尚未完全明确。我们旨在描述这种代谢性代偿。
数据取自前瞻性收集的数据库。收集患者入院时以及从高碳酸血症发生至发生后第三天的变量。对41例急性呼吸窘迫综合征患者进行分析,其中26例为持续性高碳酸血症(动脉血二氧化碳分压>50mmHg>24小时),15例为非高碳酸血症患者(对照组)。采用酸碱定量物理化学方法进行分析。
高碳酸血症组和对照组的平均年龄分别为48±18岁和44±14岁。高碳酸血症诱导后,pH值显著下降,并在随后72小时内逐渐改善,这与标准碱剩余增加一致。代谢性酸碱适应的发生是由于血清乳酸和强离子间隙降低以及无机表观强离子差增加。此外,无机表观强离子差的升高是由于血清钠、镁、钾和钙略有增加。高碳酸血症开始后72小时内血清氯未降低。
在这项解释性研究中,结果表明急性呼吸窘迫综合征患者急性持续性高碳酸血症引发的代谢性酸碱适应是复杂的。此外,高碳酸血症患者标准碱剩余的进一步快速增加涉及血清乳酸和未测定阴离子的减少,以及通过血清钠、镁、钙和钾的轻微增加导致无机表观强离子差增加。血清氯未降低。