Farris Samantha G, Zvolensky Michael J, Schmidt Norman B
Department of Psychology, The University of Houston, 126 Heyne Building, Suite 104, Houston, TX 77204-5502, USA.
Department of Psychology, The University of Houston, 126 Heyne Building, Suite 104, Houston, TX 77204-5502, USA; Department of Behavioral Science, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Cognit Ther Res. 2016 Jun;40(3):357-367. doi: 10.1007/s10608-015-9705-5. Epub 2015 Jul 19.
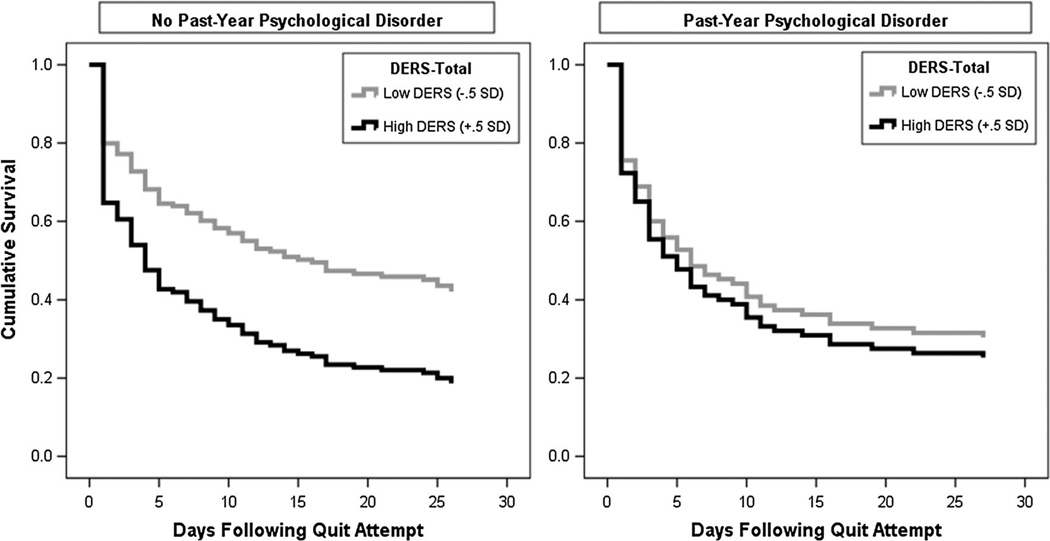
There is little knowledge about how emotion regulation difficulties interplay with psychopathology in terms of smoking cessation. Participants ( = 250; 53.2 % female, = 39.5, = 13.85) were community-recruited daily smokers (≥8 cigarettes per day) who self-reported motivation to quit smoking; 38.8 % of the sample met criteria for a current (past 12-month) psychological disorder. Emotion regulation deficits were assessed pre-quit using the Difficulties with Emotion Regulation Scale (DERS; Gratz and Roemer in J Psychopathol Behav Assess 26(1):41-54, 2004) and smoking behavior in the 28 days post-quit was assessed using the Timeline Follow-Back (TLFB; Sobell and Sobell in Measuring alcohol consumption: psychosocial and biochemical methods. Humana Press, Totowa, 1992). A Cox proportional-hazard regression analysis was used to model the effects of past-year psychopathology, DERS (total score), and their interaction, in terms of time to lapse post-quit day. After adjusting for the effects of gender, age, pre-quit level of nicotine dependence, and treatment condition, the model revealed a non-significant effect of past-year psychopathology ( = 1.14, = 0.82-1.61) and difficulties with emotion regulation ( = 1.01, = 1.00-1.01) on likelihood of lapse rate. However, the interactive effect of psychopathology status and difficulties with emotion regulation was significant ( = 0.98, = 0.97-0.99). Specifically, there was a significant conditional effect of psychopathology status on lapse rate likelihood at low, but not high, levels of emotion regulation difficulties. Plots of the cumulative survival functions indicated that for smokers without a past-year psychological disorder, those with lower DERS scores relative to elevated DERS scores had significantly lower likelihood of early smoking lapse, whereas for smokers with past-year psychopathology, DERS scores did not differentially impact lapse rate likelihood. Smokers with emotion regulation difficulties may have challenges quitting, and not having such difficulties, especially without psychopathology, decreases the potential likelihood of early lapse.
关于情绪调节困难在戒烟方面如何与精神病理学相互作用,目前所知甚少。参与者(n = 250;53.2%为女性,M = 39.5,SD = 13.85)是通过社区招募的每日吸烟者(每天≥8支香烟),他们自我报告有戒烟动机;38.8%的样本符合当前(过去12个月)心理障碍的标准。在戒烟前使用情绪调节困难量表(DERS;Gratz和Roemer,《心理病理学与行为评估杂志》,2004年,26(1):41 - 54)评估情绪调节缺陷,并使用时间线追溯法(TLFB;Sobell和Sobell,《测量酒精消费:心理社会和生化方法》,Humana Press,托托瓦,1992年)评估戒烟后28天内的吸烟行为。使用Cox比例风险回归分析来模拟过去一年的精神病理学、DERS(总分)及其相互作用对戒烟日后复吸时间的影响。在调整了性别、年龄、戒烟前尼古丁依赖水平和治疗条件的影响后,该模型显示过去一年的精神病理学(β = 1.14,95%CI = 0.82 - 1.61)和情绪调节困难(β = 1.01,95%CI = 1.00 - 1.01)对复吸率可能性的影响不显著。然而,精神病理学状态和情绪调节困难的交互作用是显著的(β = 0.98,95%CI = 0.97 - 0.99)。具体而言,在情绪调节困难程度较低而非较高时,精神病理学状态对复吸率可能性有显著的条件效应。累积生存函数图表明,对于没有过去一年心理障碍的吸烟者,DERS得分较低相对于得分较高者早期复吸的可能性显著较低,而对于有过去一年精神病理学的吸烟者,DERS得分对复吸率可能性没有差异影响。有情绪调节困难的吸烟者在戒烟时可能会面临挑战,而没有这种困难,尤其是没有精神病理学问题时,会降低早期复吸的潜在可能性。