Zimmet Alex N, Clark Matthew T, Gadrey Shrirang M, Bell Taison D, Zimmet Amanda M, Moorman J Randall, Moore Christopher C
Department of Medicine, University of Virginia School of Medicine, Charlottesville, VA.
Center for Advanced Medical Analytics, University of Virginia, Charlottesville, VA.
Crit Care Explor. 2020 Sep 23;2(10):e0191. doi: 10.1097/CCE.0000000000000191. eCollection 2020 Oct.
Bloodstream infection is associated with high mortality rates in critically ill patients but is difficult to identify clinically. This results in frequent blood culture testing, exposing patients to additional costs as well as the potential harms of unnecessary antibiotics. The purpose of this study was to assess whether the analysis of bedside physiologic monitoring data could accurately describe a pathophysiologic signature of bloodstream infection in patients admitted to the ICU.
Development of a statistical model using physiologic data from a retrospective observational cohort.
University of Virginia Medical Center (Charlottesville, VA), a tertiary-care academic medical center.
Critically ill patients consecutively admitted to either the medical or surgical/trauma ICUs with available physiologic monitoring data between February 2011 and June 2015.
None.
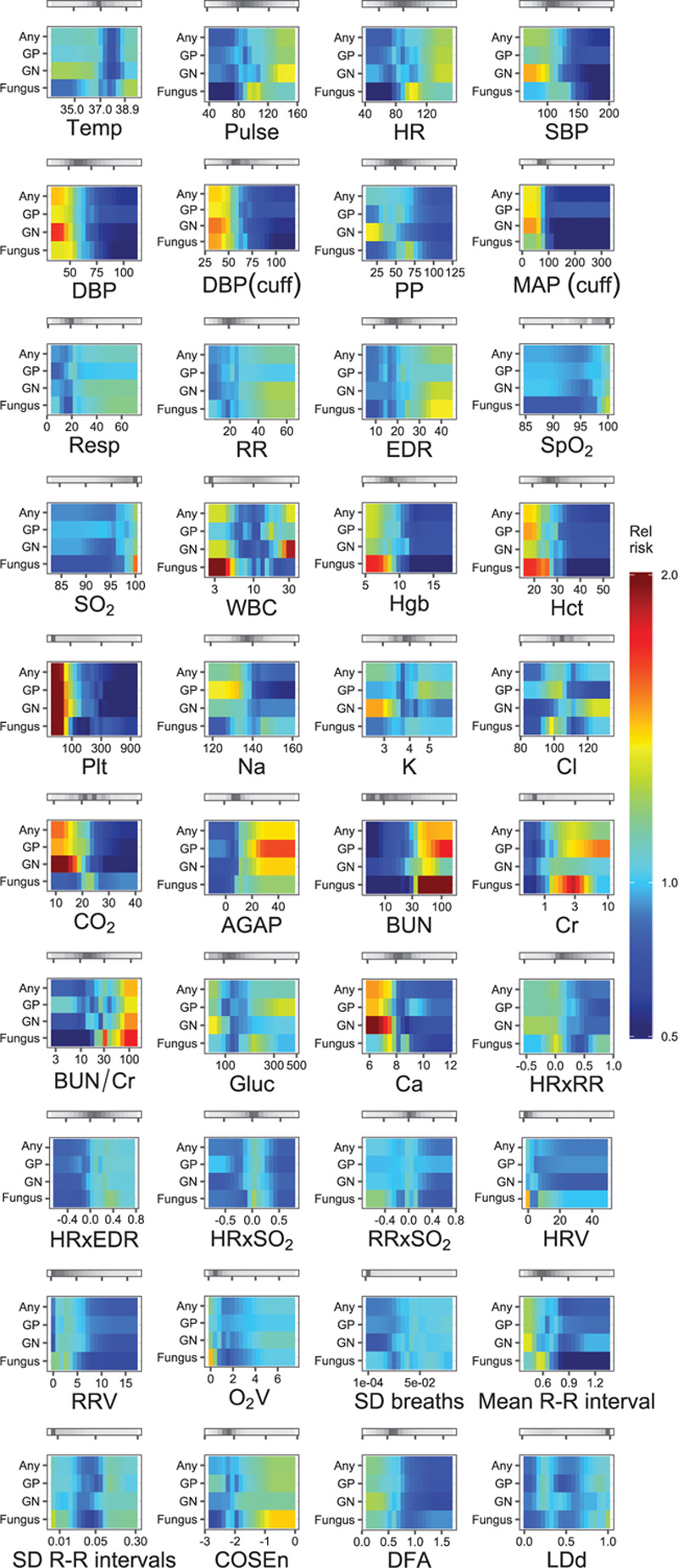
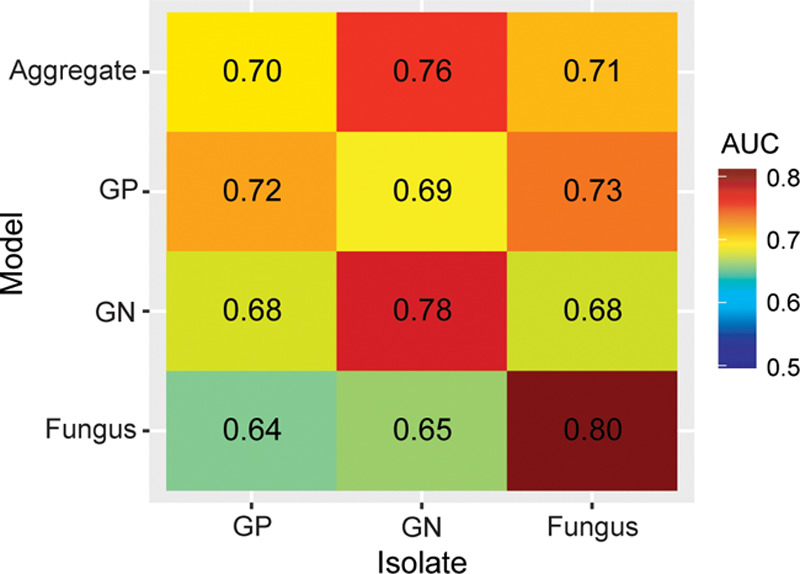
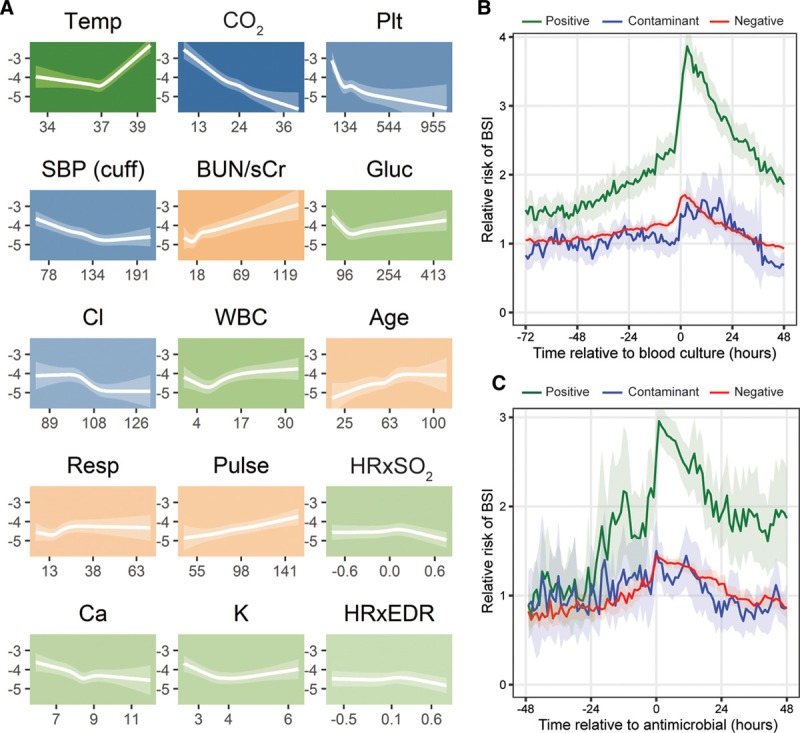
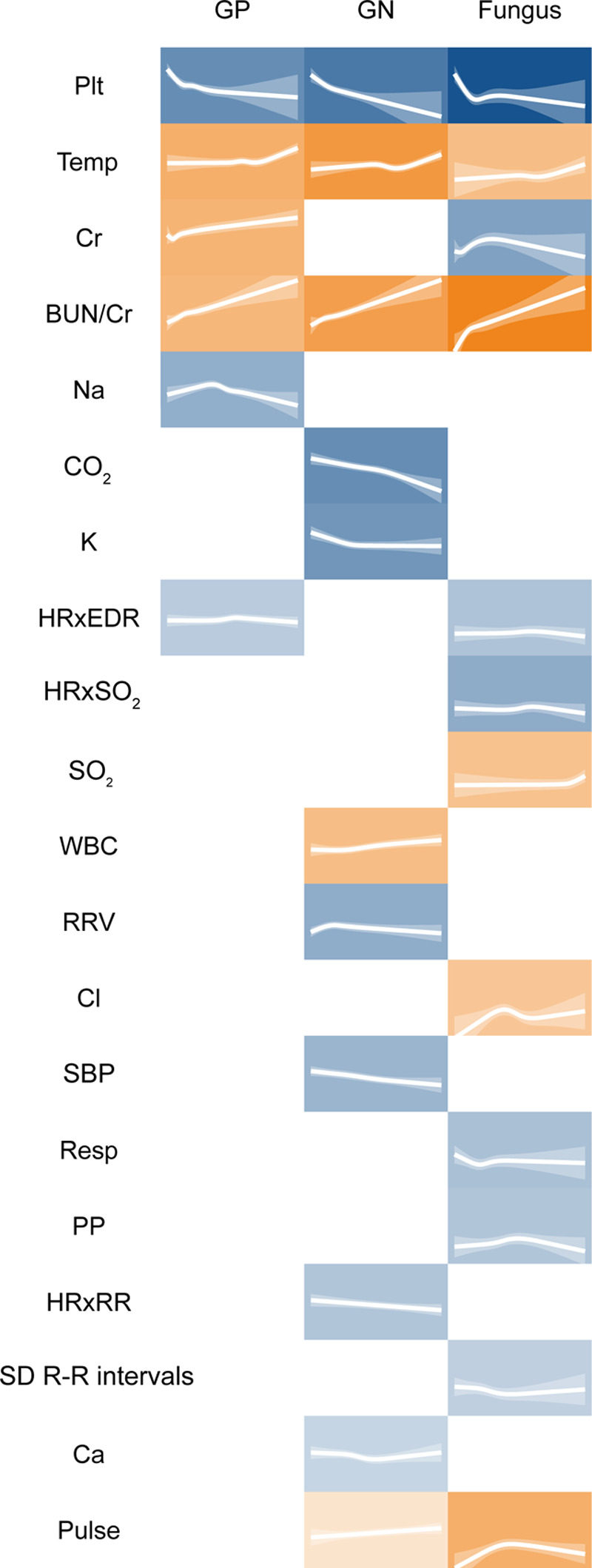
We analyzed 9,954 ICU admissions with 144 patient-years of vital sign and electrocardiography waveform data, totaling 1.3 million hourly measurements. There were 15,577 blood culture instances, with 1,184 instances of bloodstream infection (8%). The multivariate pathophysiologic signature of bloodstream infection was characterized by abnormalities in 15 different physiologic features. The cross-validated area under the receiver operating characteristic curve was 0.78 (95% CI, 0.69-0.85). We also identified distinct signatures of Gram-negative and fungal bloodstream infections, but not Gram-positive bloodstream infection.
Signatures of bloodstream infection can be identified in the routine physiologic monitoring data of critically ill adults. This may assist in identifying infected patients, maximizing diagnostic stewardship, and measuring the effect of new therapeutic modalities for sepsis.
血流感染与重症患者的高死亡率相关,但临床上难以识别。这导致频繁进行血培养检测,使患者承担额外费用以及不必要抗生素带来的潜在危害。本研究的目的是评估对床边生理监测数据的分析是否能准确描述入住重症监护病房(ICU)患者血流感染的病理生理特征。
利用回顾性观察队列的生理数据开发统计模型。
弗吉尼亚大学医学中心(弗吉尼亚州夏洛茨维尔),一家三级医疗学术医学中心。
2011年2月至2015年6月期间连续入住内科或外科/创伤ICU且有可用生理监测数据的重症患者。
无。
我们分析了9954例ICU住院病例,有144患者年的生命体征和心电图波形数据,总计130万次每小时测量。有15577次血培养情况,其中1184次为血流感染(8%)。血流感染的多变量病理生理特征表现为15种不同生理特征异常。受试者工作特征曲线下的交叉验证面积为0.78(95%CI,0.69 - 0.85)。我们还确定了革兰阴性菌和真菌血流感染的不同特征,但未确定革兰阳性菌血流感染的特征。
在重症成年患者的常规生理监测数据中可识别出血流感染的特征。这可能有助于识别感染患者、优化诊断管理以及评估脓毒症新治疗方式的效果。