Armstrong Corinne E, Martínez-Álvarez Melisa, Singh Neha S, John Theopista, Afnan-Holmes Hoviyeh, Grundy Chris, Ruktanochai Corrine W, Borghi Josephine, Magoma Moke, Msemo Georgina, Matthews Zoe, Mtei Gemini, Lawn Joy E
Centre for Maternal, Adolescent, Reproductive and Child Health, London School of Hygiene & Tropical Medicine, London, WC1E 7HT, UK.
Evidence for Action, Dar es Salaam, Tanzania.
BMC Public Health. 2016 Sep 12;16 Suppl 2(Suppl 2):795. doi: 10.1186/s12889-016-3404-3.
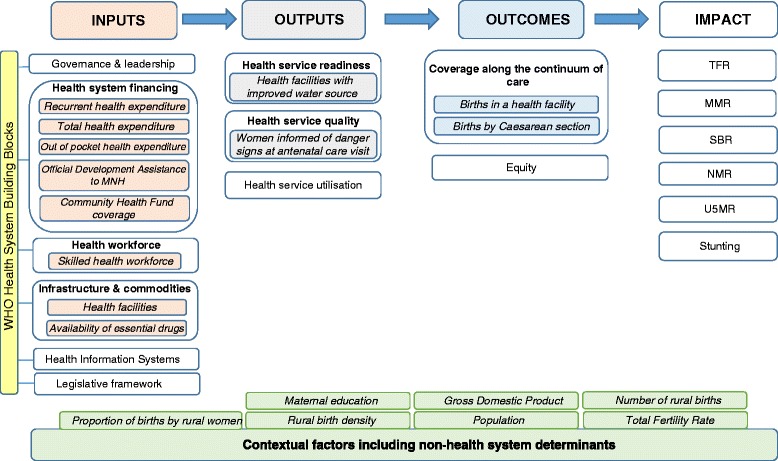
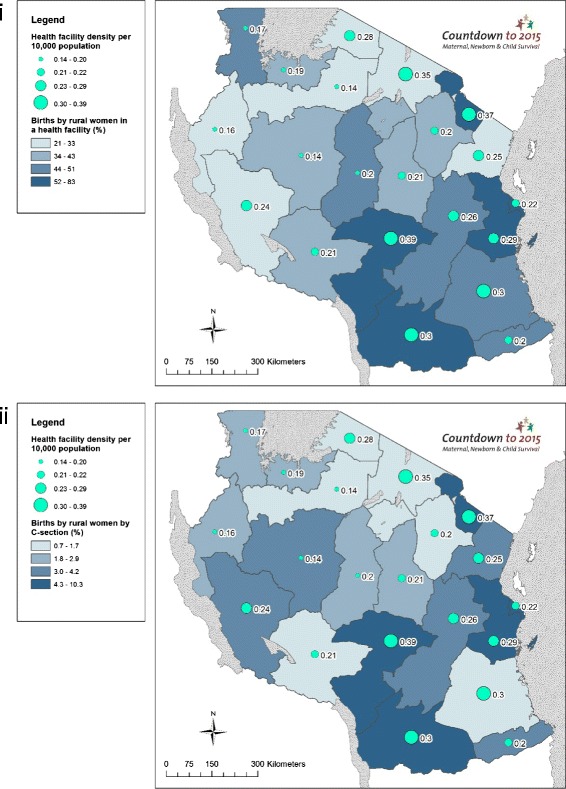
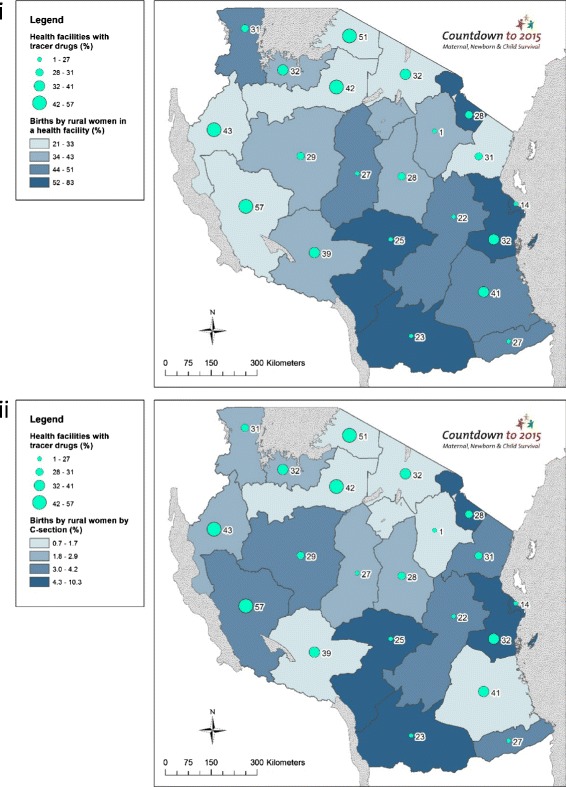
Tanzania achieved the Millennium Development Goal for child survival, yet made insufficient progress for maternal and neonatal survival and stillbirths, due to low coverage and quality of services for care at birth, with rural women left behind. Our study aimed to evaluate Tanzania's subnational (regional-level) variations for rural care at birth outcomes, i.e., rural women giving birth in a facility and by Caesarean section (C-section), and associations with health systems inputs (financing, health workforce, facilities, and commodities), outputs (readiness and quality of care) and context (education and GDP).
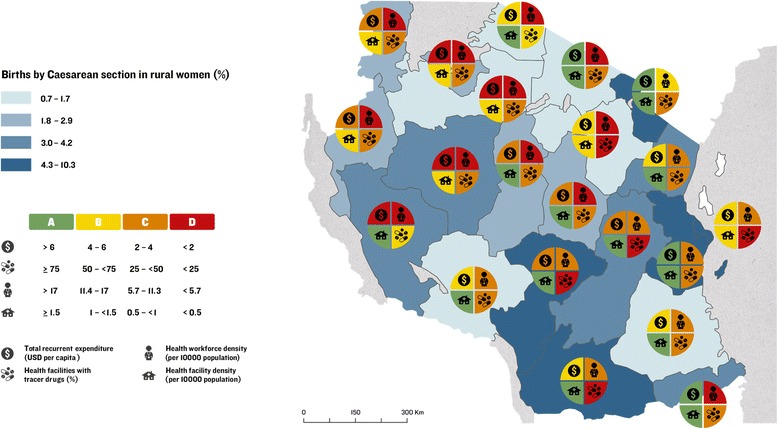
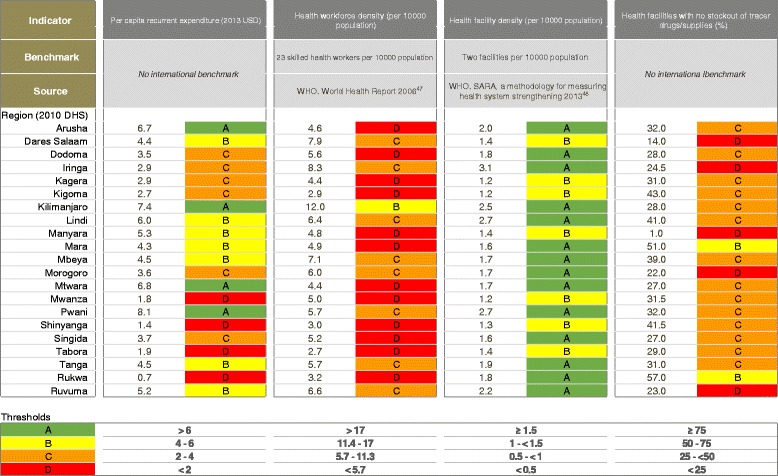
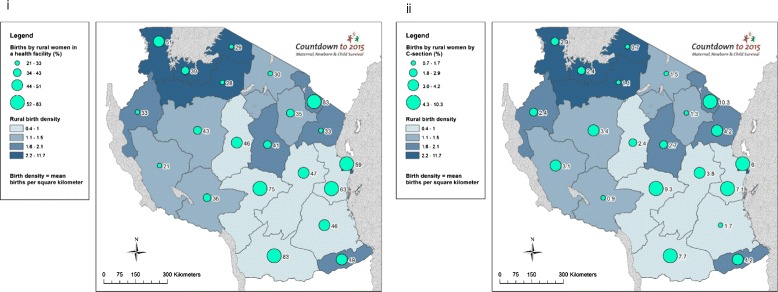
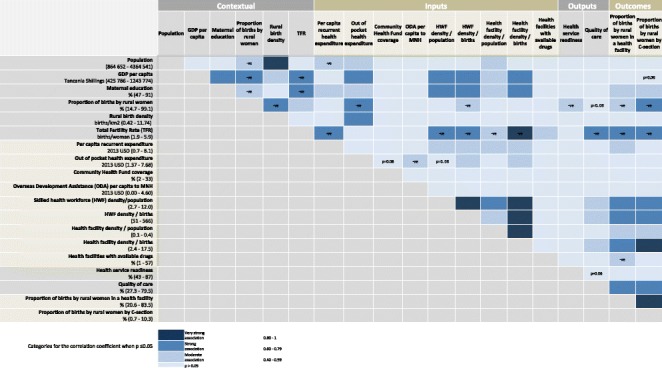
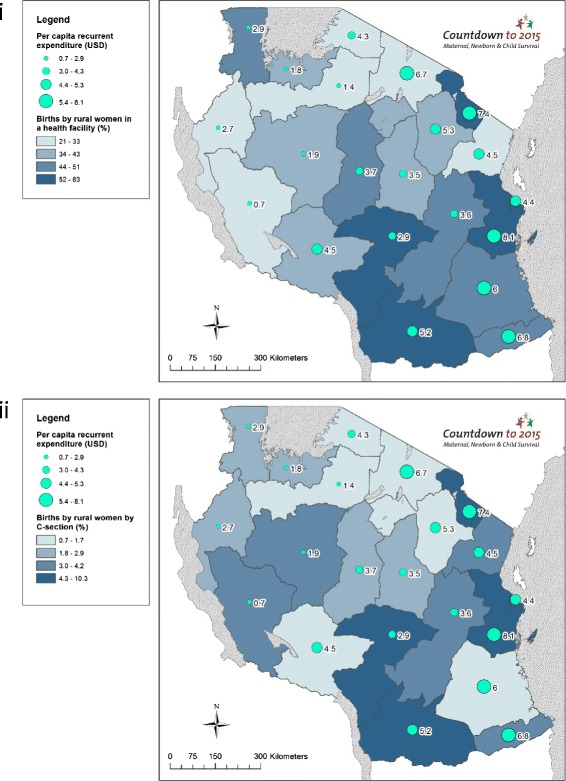
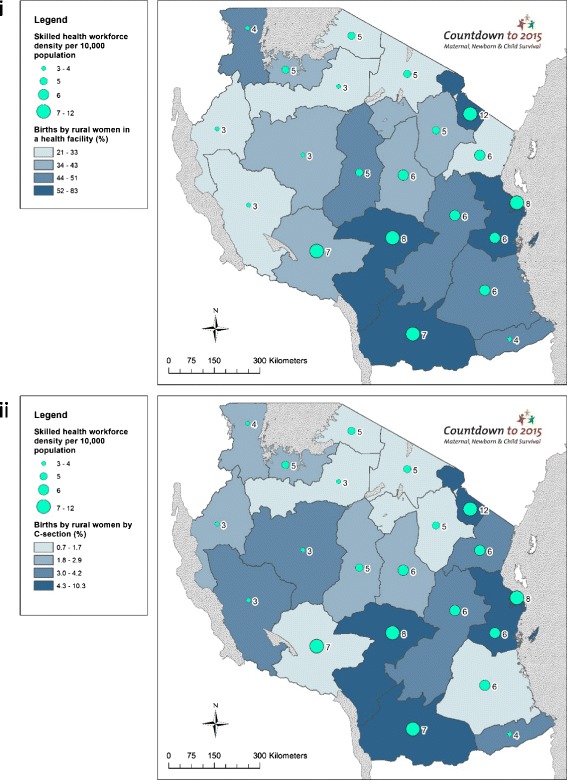
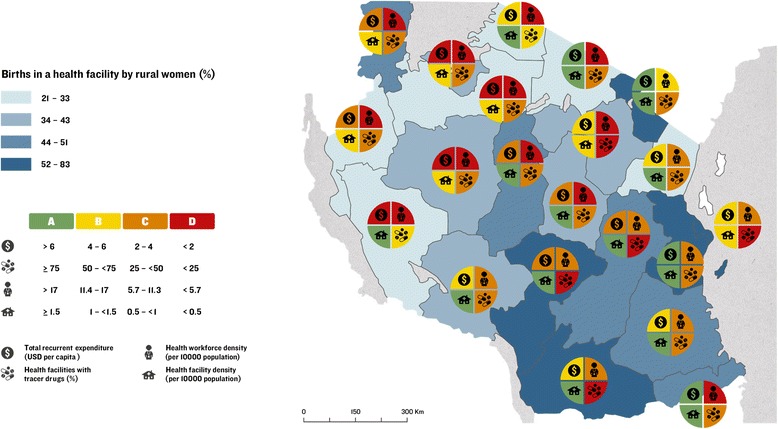
We undertook correlation analyses of subnational-level associations between health system inputs, outputs, context, and rural care at birth outcomes; and constructed implementation readiness barometers using benchmarks for each health system input indicator. We used geographical information system (GIS) mapping to visualise subnational variations in care at birth for rural women, with a focus on service availability and readiness, and collected qualitative data to investigate financial flows from national to council level to understand variation in financing inputs.
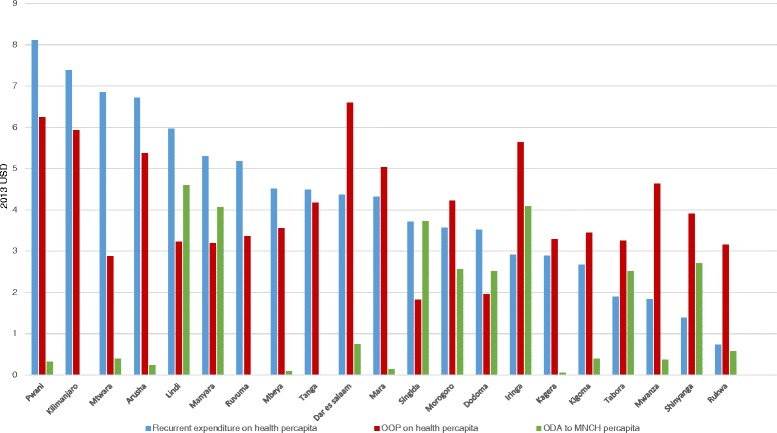
We found wide subnational variation for rural care at birth outcomes, health systems inputs, and contextual indicators. There was a positive association between rural women giving birth in a facility and by C-section; maternal education; workforce and facility density; and quality of care. There was a negative association between these outcomes and proportion of all births to rural women, total fertility rate, and availability of essential commodities at facilities. Per capita recurrent expenditure was positively associated with facility births (correlation coefficient = 0.43; p = 0.05) but not with C-section. Qualitative results showed that the health financing system is complex and insufficient for providing care at birth services. Bottlenecks for care at birth included low density of health workers, poor availability of essential commodities, and low health financing in Lake and Western Zones.
No region meets the benchmarks for the four health systems building blocks including health finance, health workforce, health facilities, and commodities. Strategies for addressing health system inequities, including overall increases in health expenditure, are needed in rural populations and areas of highest unmet need for family planning to improve coverage of care at birth for rural women in Tanzania.
坦桑尼亚实现了儿童生存方面的千年发展目标,但在孕产妇和新生儿生存及死产方面进展不足,原因是出生护理服务的覆盖范围和质量较低,农村妇女被落下。我们的研究旨在评估坦桑尼亚次国家级(区域层面)农村出生护理结果的差异,即农村妇女在医疗机构分娩和剖宫产的情况,以及与卫生系统投入(融资、卫生人力、设施和商品)、产出(准备情况和护理质量)和背景(教育和国内生产总值)之间的关联。
我们对卫生系统投入、产出、背景与农村出生护理结果之间的次国家级关联进行了相关性分析;并使用每个卫生系统投入指标的基准构建了实施准备情况晴雨表。我们使用地理信息系统(GIS)绘图来直观呈现农村妇女出生护理的次国家级差异,重点关注服务的可及性和准备情况,并收集定性数据以调查从国家到地方议会层面的资金流动情况,以了解融资投入的差异。
我们发现农村出生护理结果、卫生系统投入和背景指标在次国家级层面存在很大差异。农村妇女在医疗机构分娩和剖宫产之间存在正相关;孕产妇教育;卫生人力和设施密度;以及护理质量。这些结果与农村妇女分娩总数的比例、总生育率以及医疗机构基本商品的可及性之间存在负相关。人均经常性支出与医疗机构分娩呈正相关(相关系数 = 0.43;p = 0.05),但与剖宫产无关。定性结果表明,卫生融资系统复杂且不足以提供出生护理服务。出生护理的瓶颈包括卫生工作者密度低、基本商品可及性差以及湖泊和西区卫生融资水平低。
没有一个地区达到包括卫生融资、卫生人力、卫生设施和商品在内的四个卫生系统组成部分的基准。需要采取战略来解决卫生系统不平等问题,包括总体增加卫生支出,在农村人口和计划生育需求未得到满足程度最高的地区,以提高坦桑尼亚农村妇女出生护理的覆盖率。