Hunma S, Ramuth H, Miles-Chan J L, Schutz Y, Montani J-P, Joonas N, Dulloo A G
Obesity Unit, Victoria Hospital, Candos, Mauritius.
Division of Physiology, Department of Medicine, University of Fribourg, Fribourg, Switzerland.
Int J Obes (Lond). 2016 Dec;40(12):1906-1914. doi: 10.1038/ijo.2016.176. Epub 2016 Oct 4.
Global estimates of overweight and obesity prevalence are based on the World Health Organisation (WHO) body mass index (BMI) cut-off values of 25 and 30 kg m, respectively. To validate these BMI cut-offs for adiposity in the island population of Mauritius, we assessed the relationship between BMI and measured body fat mass in this population according to gender and ethnicity.
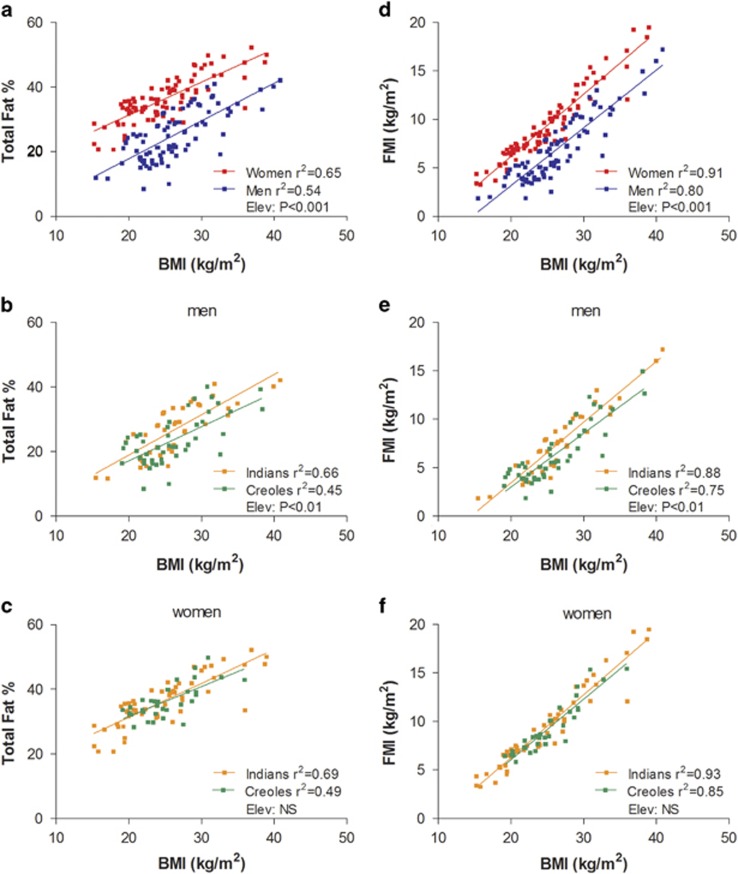
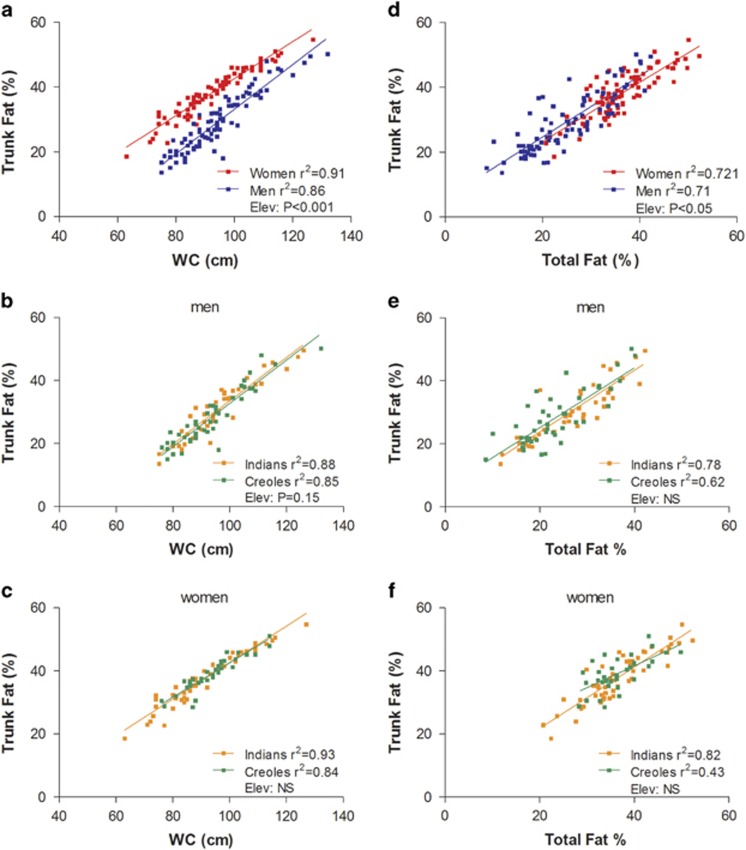
In 175 young adult Mauritians (age 20-42 years) belonging to the two main ethnic groups-Indians (South Asian descent) and Creoles (African/Malagasy descent), body weight, height and waist circumference (WC) were measured, total body fat assessed by deuterium oxide (D2O) dilution and trunk (abdominal) fat by segmental bioimpedance analysis.
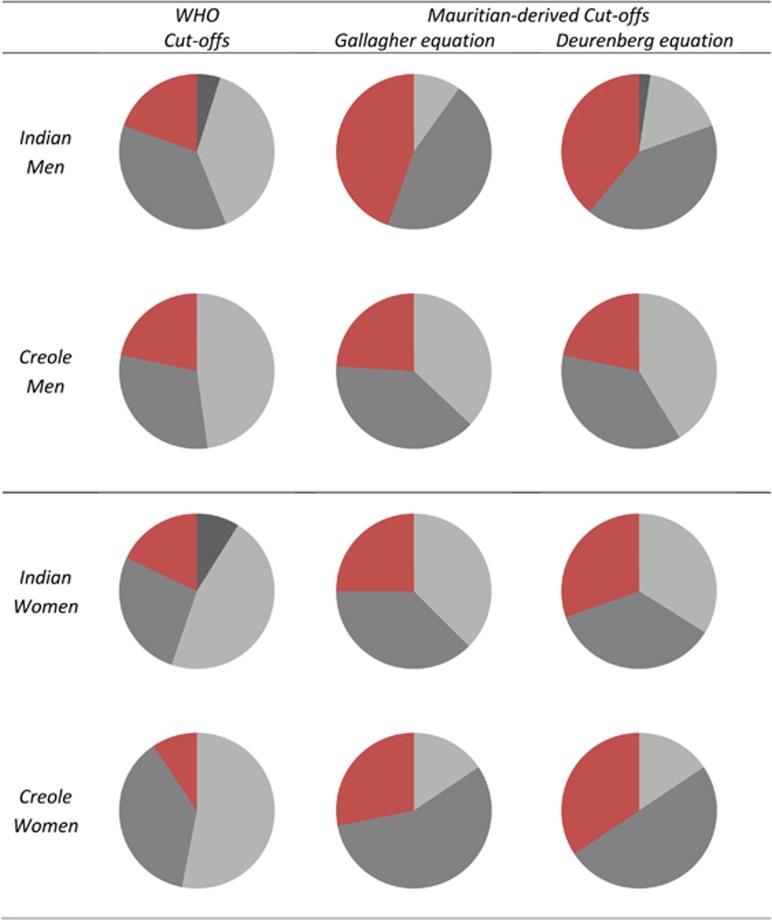
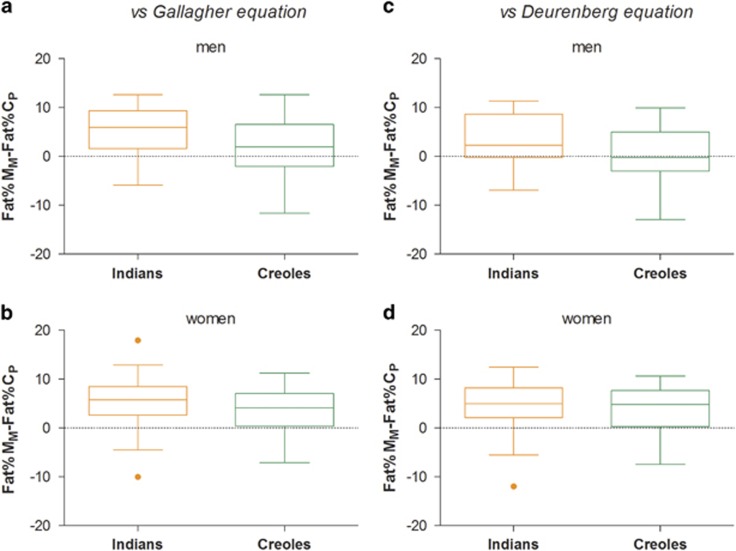
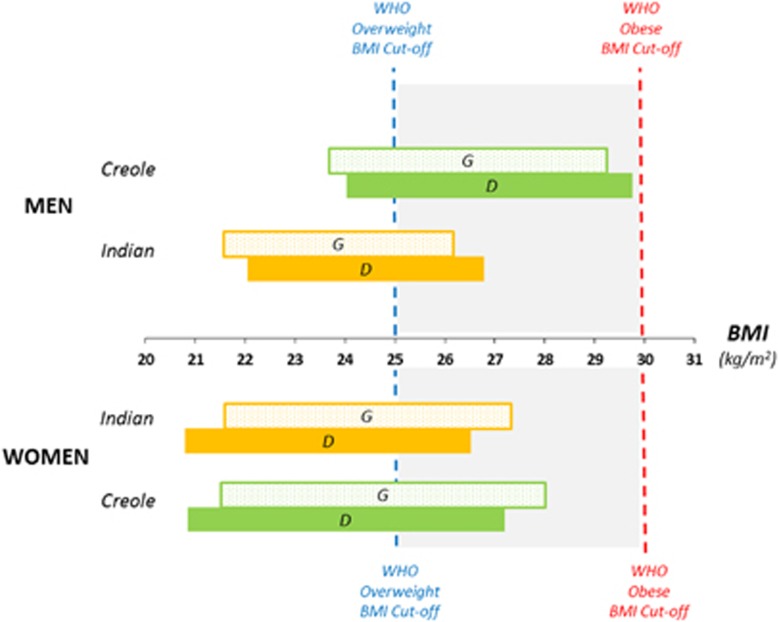
Compared to body fat% predicted from BMI using Caucasian-based equations, body fat% assessed by D2O dilution in Mauritians was higher by 3-5 units in Indian men and women as well as in Creole women, but not in Creole men. This gender-specific ethnic difference in body composition between Indians and Creoles is reflected in their BMI-Fat% relationships, as well as in their WC-Trunk Fat% relationships. Overall, WHO BMI cut-offs of 25 and 30 kg m for overweight and obesity, respectively, seem valid only for Creole men (~24 and 29.5, respectively), but not for Creole women whose BMI cut-offs are 2-4 units lower (21-22 for overweight; 27-28 for obese) nor for Indian men and women whose BMI cut-offs are 3-4 units lower (21-22 for overweight; 26-27 for obese).
The use of BMI cut-off points for classifying overweight and obesity need to take into account both ethnicity and gender to avoid gross adiposity status misclassification in this population known to be at high risk for type-2 diabetes and cardiovascular diseases. This is particularly of importance in obesity prevention strategies both in clinical medicine and public health.
全球超重和肥胖患病率的估计是基于世界卫生组织(WHO)的体重指数(BMI)临界值,分别为25和30kg/m²。为验证这些BMI临界值在毛里求斯岛人群中用于评估肥胖程度的有效性,我们根据性别和种族评估了该人群中BMI与实测体脂量之间的关系。
在175名20至42岁的毛里求斯年轻成年人中,他们分属两个主要种族——印度人(南亚血统)和克里奥尔人(非洲/马达加斯加血统),测量了体重、身高和腰围(WC),通过氧化氘(D2O)稀释法评估全身脂肪,并通过分段生物电阻抗分析评估躯干(腹部)脂肪。
与使用基于白种人的公式从BMI预测的体脂百分比相比,毛里求斯人中通过D2O稀释法评估的体脂百分比在印度男性和女性以及克里奥尔女性中比预测值高3至5个百分点,但在克里奥尔男性中并非如此。印度人和克里奥尔人在身体组成上这种特定性别的种族差异反映在他们的BMI-体脂百分比关系以及腰围-躯干脂肪百分比关系中。总体而言,WHO的超重和肥胖BMI临界值分别为25和30kg/m²,似乎仅对克里奥尔男性有效(分别约为24和29.5),但对克里奥尔女性无效,其BMI临界值低2至4个百分点(超重为21至22;肥胖为27至28),对印度男性和女性也无效,其BMI临界值低3至4个百分点(超重为21至22;肥胖为26至27)。
使用BMI临界值对超重和肥胖进行分类时需要考虑种族和性别,以避免在这个已知患2型糖尿病和心血管疾病风险较高的人群中出现肥胖程度的严重误判。这在临床医学和公共卫生的肥胖预防策略中尤为重要。