Hori Tomohide, Oike Fumitaka, Furuyama Hiroaki, Machimoto Takafumi, Kadokawa Yoshio, Hata Toshiyuki, Kato Shigeru, Yasukawa Daiki, Aisu Yuki, Sasaki Maho, Kimura Yusuke, Takamatsu Yuichiro, Naito Masato, Nakauchi Masaya, Tanaka Takahiro, Gunji Daigo, Nakamura Kiyokuni, Sato Kiyoko, Mizuno Masahiro, Iida Taku, Yagi Shintaro, Uemoto Shinji, Yoshimura Tsunehiro
Tomohide Hori, Hiroaki Furuyama, Takafumi Machimoto, Yoshio Kadokawa, Toshiyuki Hata, Shigeru Kato, Daiki Yasukawa, Yuki Aisu, Maho Sasaki, Yusuke Kimura, Yuichiro Takamatsu, Tsunehiro Yoshimura, Department of Gastrointestinal and General Surgery, Tenriyorodusoudanjyo Hospital, Tenri 632-8552, Japan.
World J Gastroenterol. 2016 Dec 21;22(47):10287-10303. doi: 10.3748/wjg.v22.i47.10287.
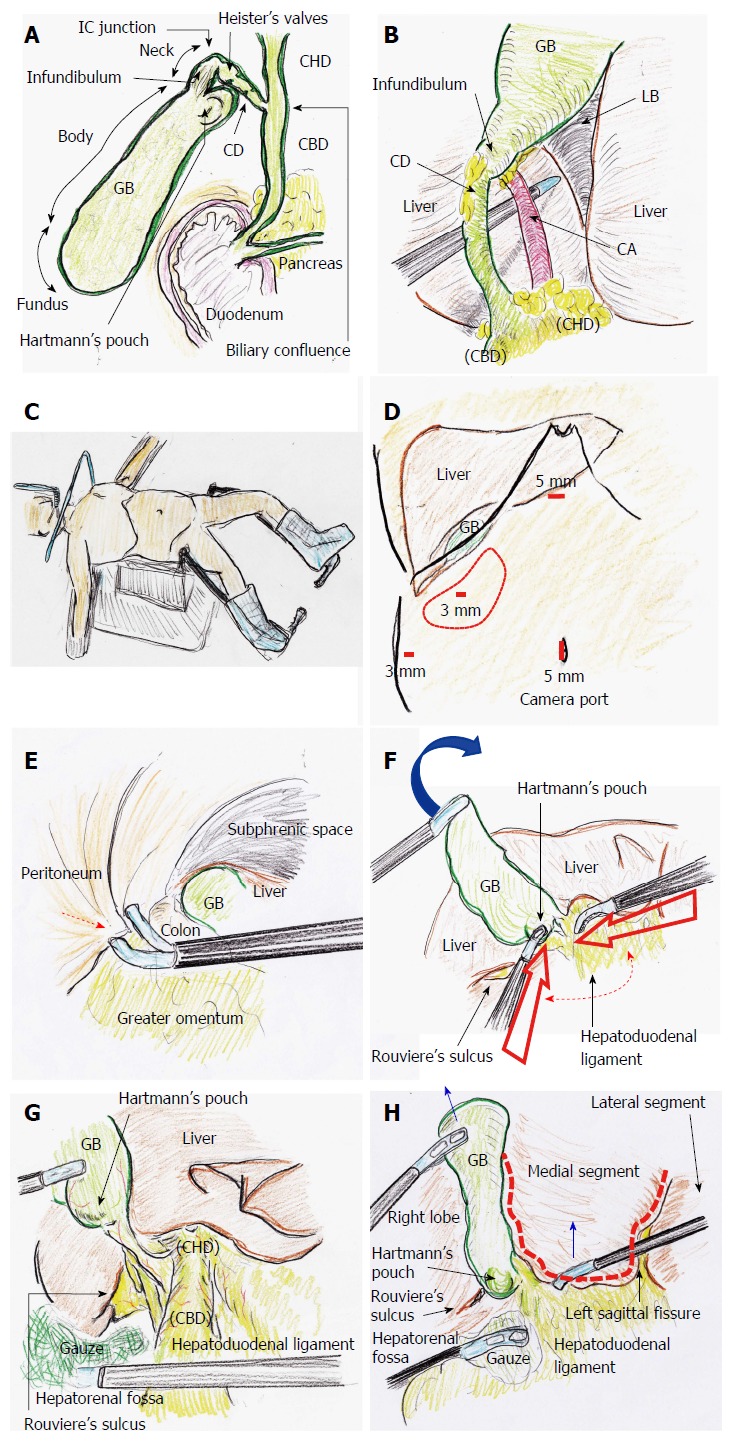
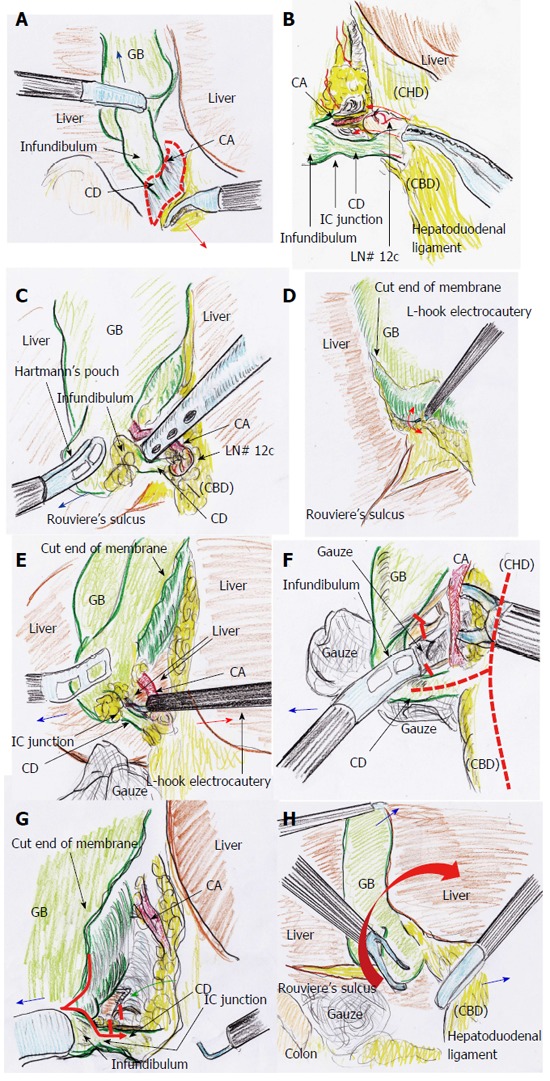
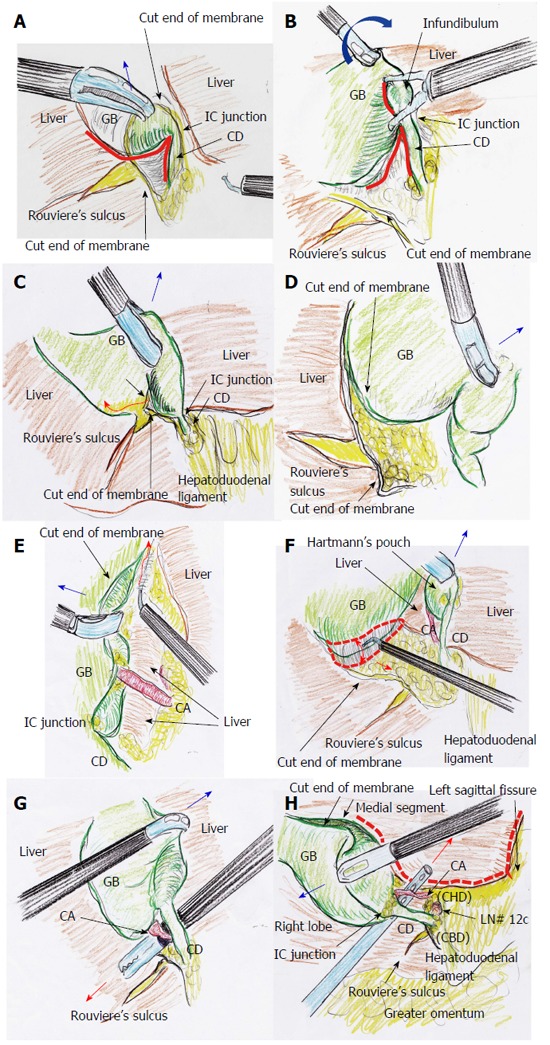
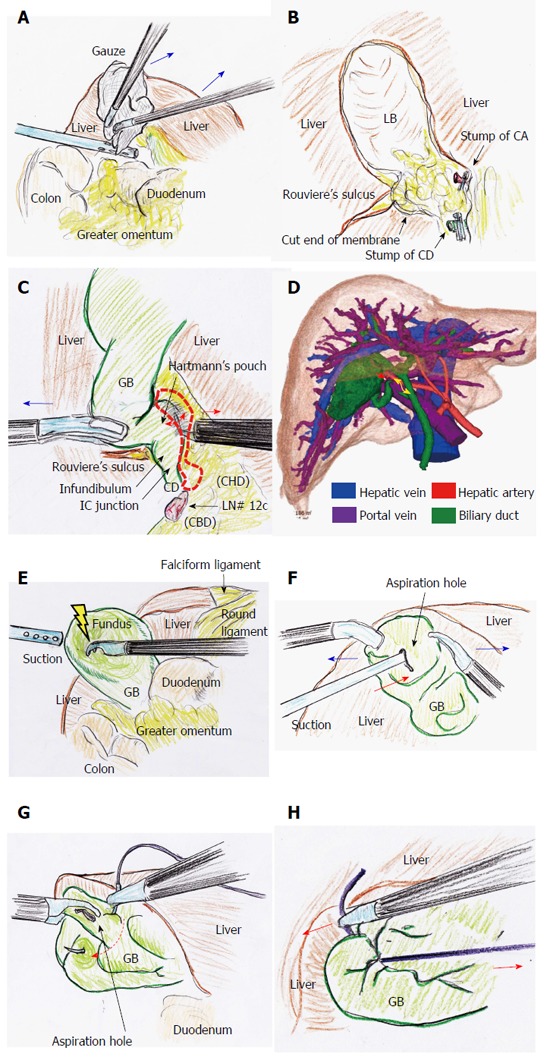
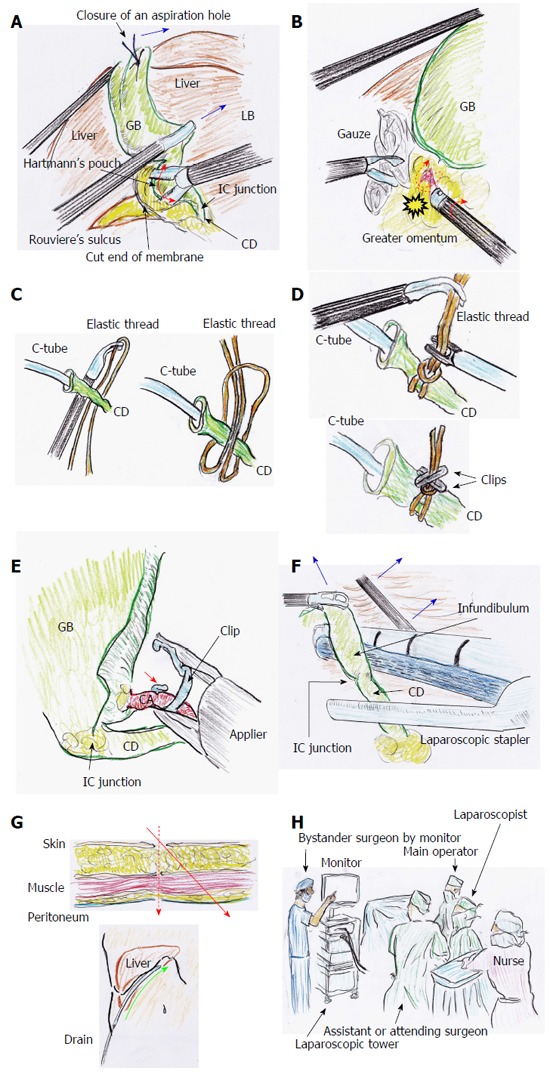
Laparoscopic cholecystectomy (LC) does not require advanced techniques, and its performance has therefore rapidly spread worldwide. However, the rate of biliary injuries has not decreased. The concept of the critical view of safety (CVS) was first documented two decades ago. Unexpected injuries are principally due to misidentification of human factors. The surgeon's assumption is a major cause of misidentification, and a high level of experience alone is not sufficient for successful LC. We herein describe tips and pitfalls of LC in detail and discuss various technical considerations. Finally, based on a review of important papers and our own experience, we summarize the following mandatory protocol for safe LC: (1) consideration that a high level of experience alone is not enough; (2) recognition of the plateau involving the common hepatic duct and hepatic hilum; (3) blunt dissection until CVS exposure; (4) Calot's triangle clearance in the overhead view; (5) Calot's triangle clearance in the view from underneath; (6) dissection of the posterior right side of Calot's triangle; (7) removal of the gallbladder body; and (8) positive CVS exposure. We believe that adherence to this protocol will ensure successful and beneficial LC worldwide, even in patients with inflammatory changes and rare anatomies.
腹腔镜胆囊切除术(LC)并不需要先进的技术,因此其应用已在全球迅速普及。然而,胆管损伤的发生率并未降低。安全关键视野(CVS)的概念在二十年前首次被记录。意外损伤主要是由于人为因素的误判。外科医生的主观臆断是误判的主要原因,仅凭丰富的经验不足以成功实施LC。我们在此详细描述LC的技巧与陷阱,并讨论各种技术要点。最后,基于对重要文献的回顾以及我们自己的经验,我们总结出以下安全LC的强制性操作流程:(1)认识到仅凭丰富经验是不够的;(2)识别涉及肝总管和肝门的平台;(3)钝性分离直至暴露CVS;(4)从上方观察时清理胆囊三角;(5)从下方观察时清理胆囊三角;(6)解剖胆囊三角的右后侧;(7)切除胆囊体;(8)确保CVS清晰暴露。我们相信,遵循这一操作流程将确保在全球范围内成功且有益地实施LC,即使是对于有炎症改变和罕见解剖结构的患者。