Chacaroun Samarmar, Borowik Anna, Morrison Shawnda A, Baillieul Sébastien, Flore Patrice, Doutreleau Stéphane, Verges Samuel
HP2 Laboratory, University Grenoble AlpesGrenoble, France; U1042, Institut National de la Santé et de la Recherche MédicaleGrenoble, France.
Applied Kinesiology, University of Primorska Primorska, Slovenia.
Front Physiol. 2017 Jan 10;7:675. doi: 10.3389/fphys.2016.00675. eCollection 2016.
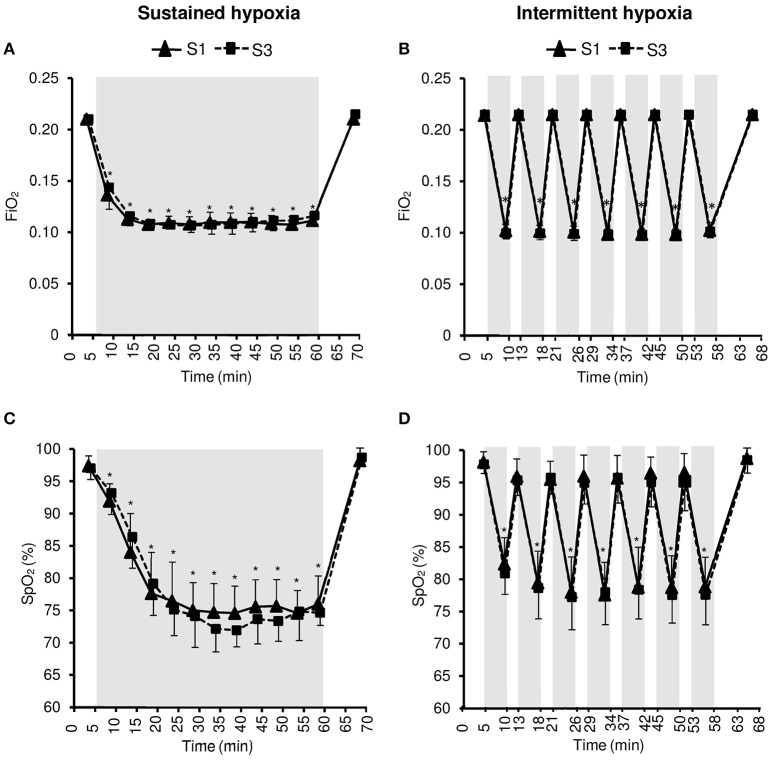
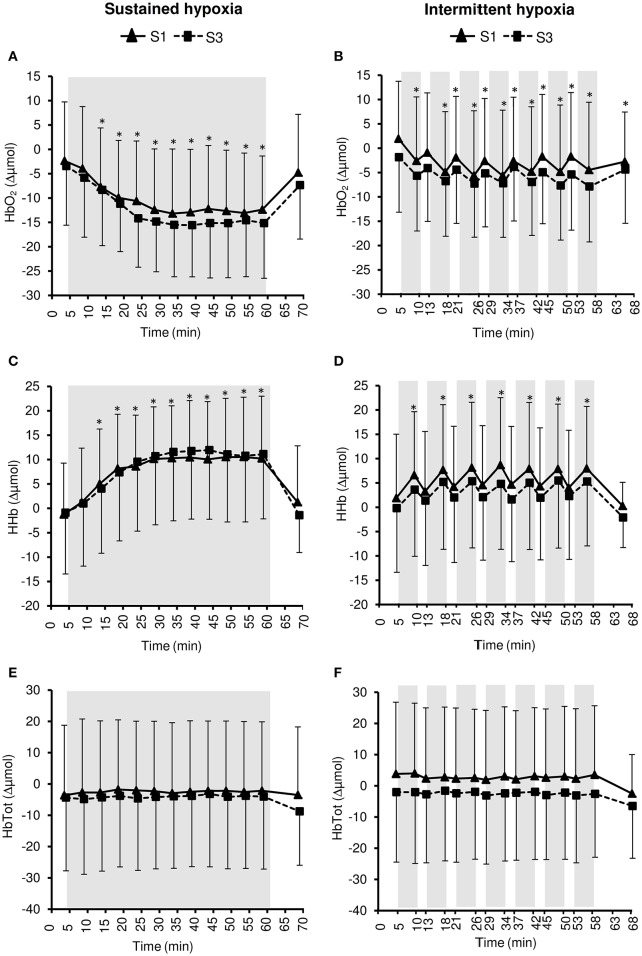
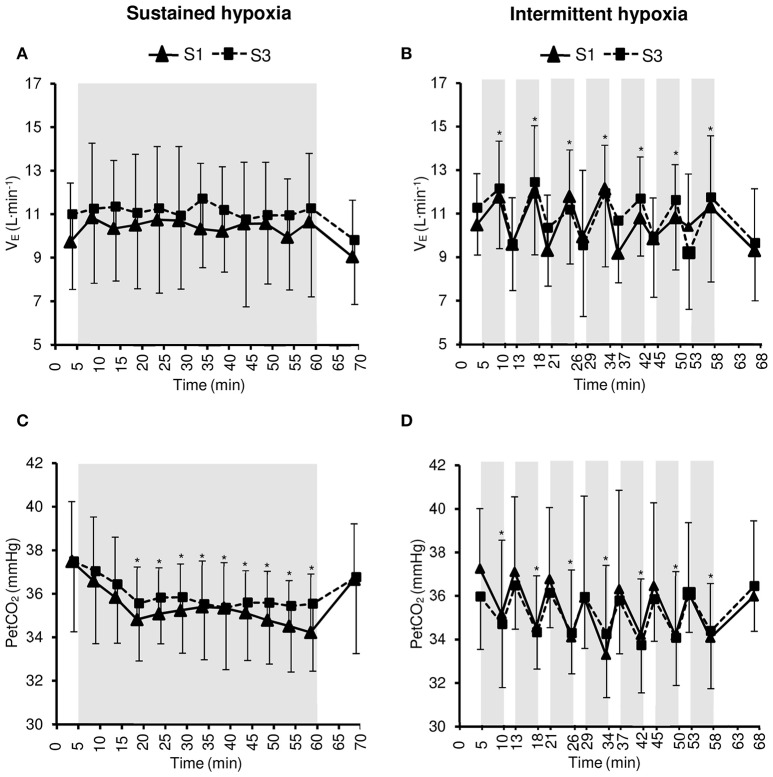
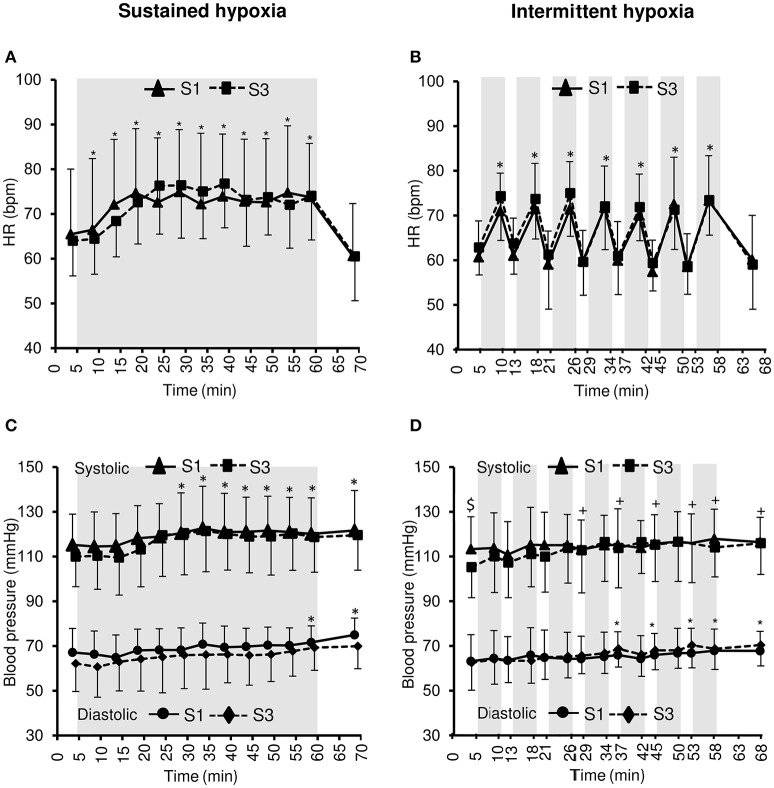
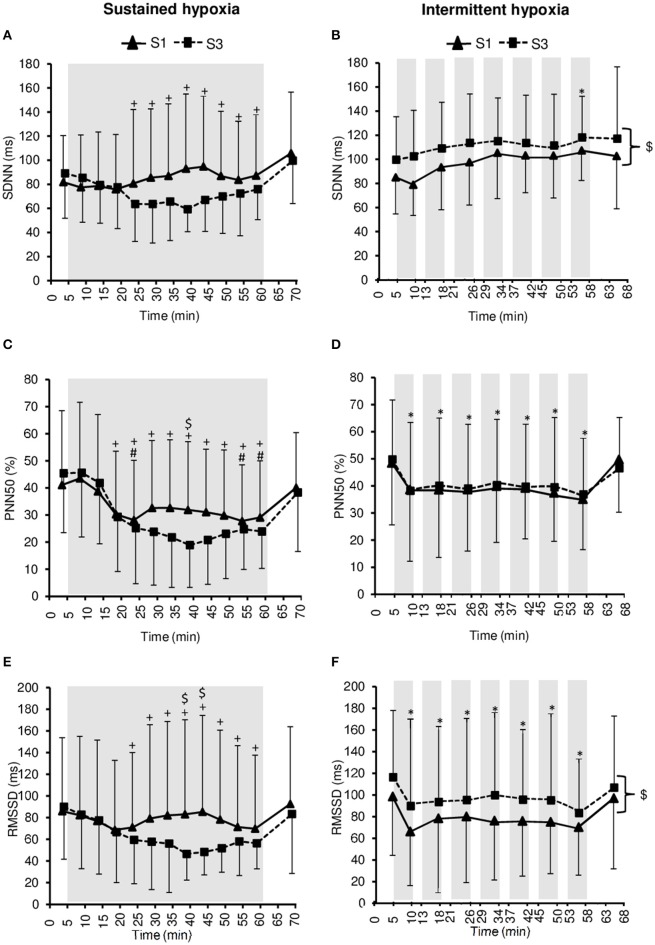
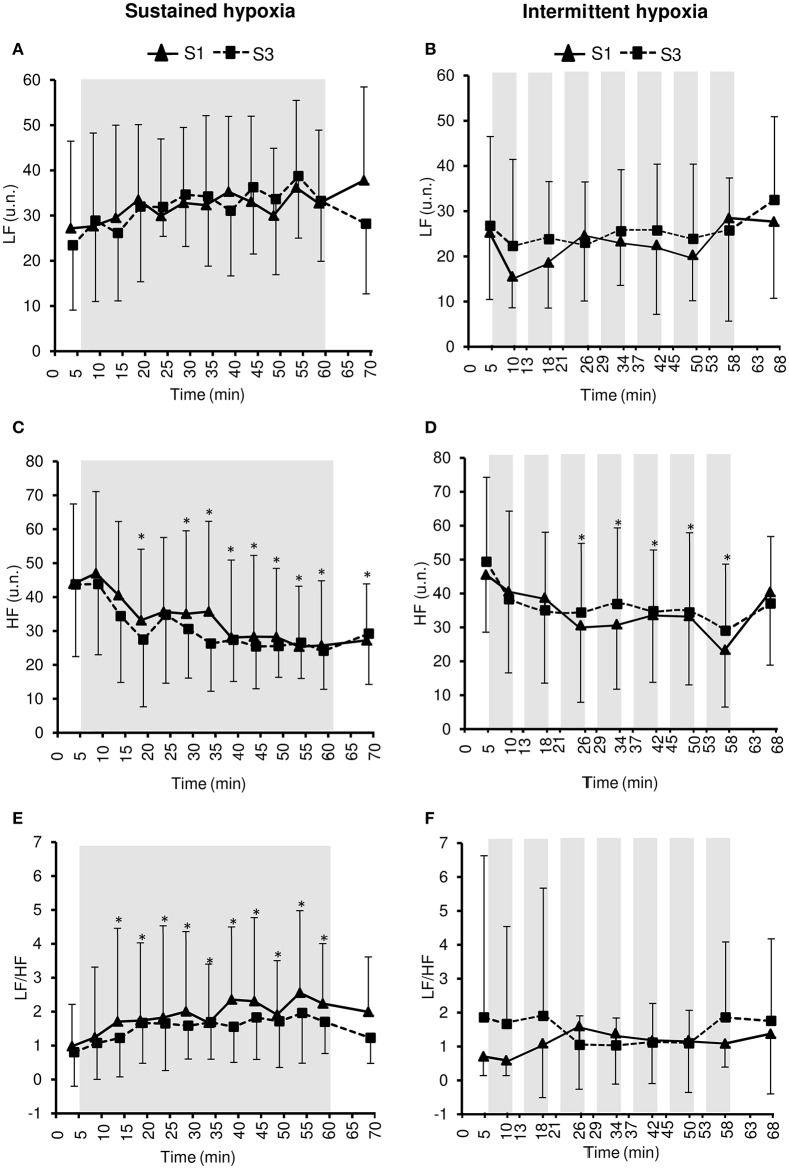
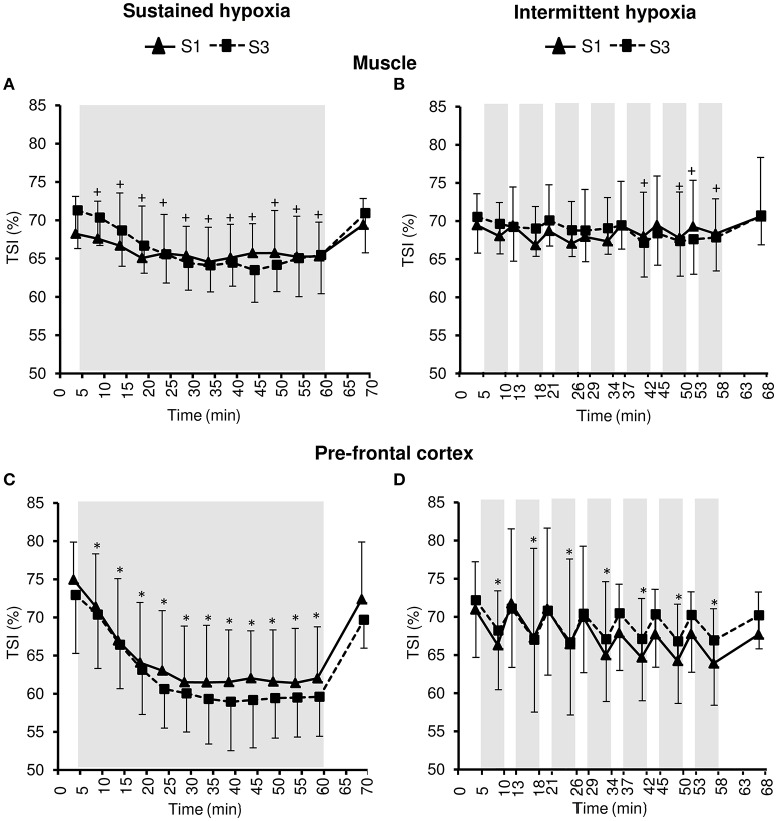
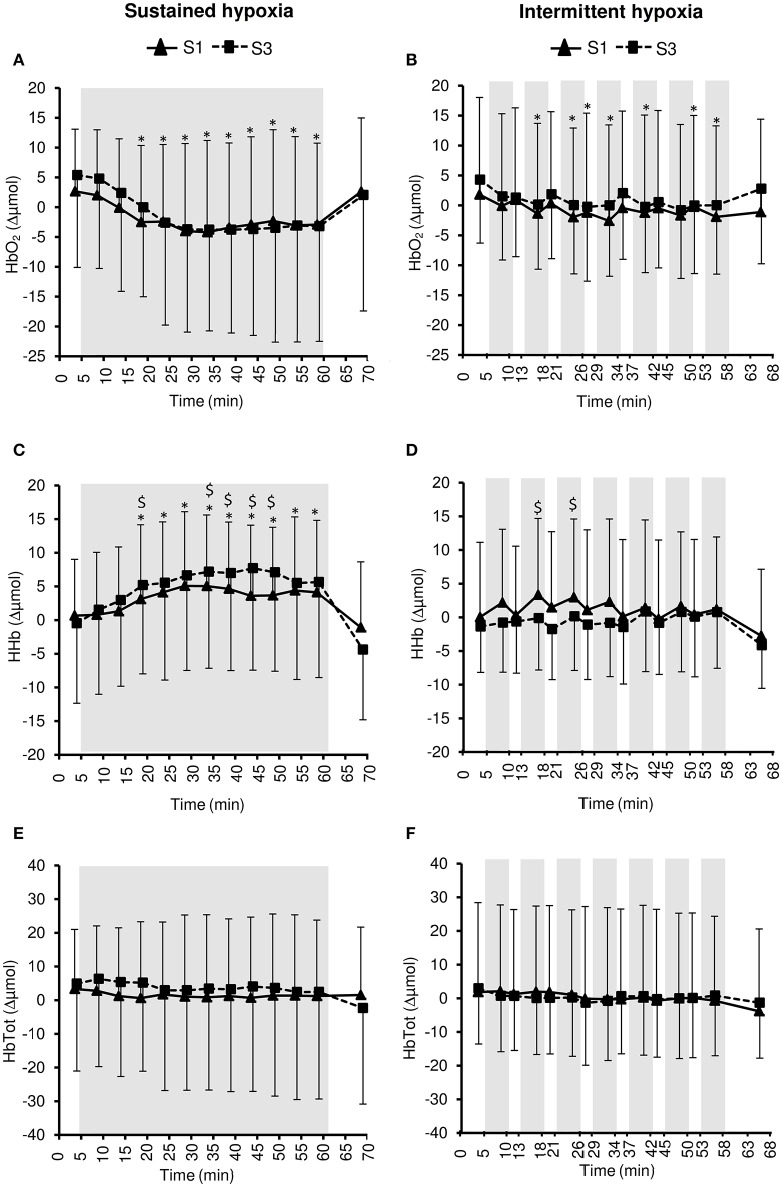
Hypoxic exposure can be used as a therapeutic tool by inducing various cardiovascular, neuromuscular, and metabolic adaptations. Hypoxic conditioning strategies have been evaluated in patients with chronic diseases using either sustained (SH) or intermittent (IH) hypoxic sessions. Whether hypoxic conditioning via SH or IH may induce different physiological responses remains to be elucidated. Fourteen healthy active subjects (7 females, age 25 ± 8 years, body mass index 21.5 ± 2.5 kg·m) performed two interventions in a single blind, randomized cross-over design, starting with either 3 x SH (48 h apart), or 3 x IH (48 h apart), separated by a 2 week washout period. SH sessions consisted of breathing a gas mixture with reduced inspiratory oxygen fraction (FiO), continuously adjusted to reach arterial oxygen saturations (SpO) of 70-80% for 1 h. IH sessions consisted of 5 min with reduced FiO (SpO = 70-80%), followed by 3-min normoxia, repeated seven times. During the first (S1) and third (S3) sessions of each hypoxic intervention, cardiorespiratory parameters, and muscle and pre-frontal cortex oxygenation (near infrared spectroscopy) were assessed continuously. : Minute ventilation increased significantly during IH sessions (+2 ± 2 L·min) while heart rate increased during both SH (+11 ± 4 bpm) and IH (+13 ± 5 bpm) sessions. Arterial blood pressure increased during all hypoxic sessions, although baseline normoxic systolic blood pressure was reduced from S1 to S3 in IH only (-8 ± 11 mmHg). Muscle oxygenation decreased significantly during S3 but not S1, for both hypoxic interventions (S3: SH -6 ± 5%, IH -3 ± 4%); pre-frontal oxygenation decreased in S1 and S3, and to a greater extent in SH vs. IH (-13 ± 3% vs. -6 ± 6%). Heart rate variability indices indicated a significantly larger increase in sympathetic activity in SH vs. IH (lower SDNN, PNN50, and RMSSD values in SH). From S1 to S3, further reduction in heart rate variability was observed in SH (SDNN, PNN50, and RMSSD reduction) while heart rate variability increased in IH (SDNN and RMSSD increase). These results showed significant differences in heart rate variability, blood pressure, and tissue oxygenation changes during short-term SH vs. IH conditioning interventions. Heart rate variability may provide useful information about the early adaptations induced by such intervention.
缺氧暴露可通过诱导各种心血管、神经肌肉和代谢适应,用作一种治疗手段。已使用持续(SH)或间歇性(IH)缺氧疗程,对患有慢性病的患者进行缺氧预处理策略评估。通过SH或IH进行的缺氧预处理是否会诱导不同的生理反应,仍有待阐明。14名健康的活跃受试者(7名女性,年龄25±8岁,体重指数21.5±2.5kg·m)采用单盲、随机交叉设计进行了两项干预,要么从3次SH(间隔48小时)开始,要么从3次IH(间隔48小时)开始,中间有2周的洗脱期。SH疗程包括呼吸一种吸入氧分数(FiO)降低的混合气体,持续调整以达到动脉血氧饱和度(SpO)为70 - 80%,持续1小时。IH疗程包括5分钟FiO降低(SpO = 70 - 80%),随后3分钟常氧,重复7次。在每次缺氧干预的第一次(S1)和第三次(S3)疗程中,连续评估心肺参数以及肌肉和前额叶皮质的氧合情况(近红外光谱法)。:IH疗程期间分钟通气量显著增加(+2±2L·min),而SH(+11±4bpm)和IH(+13±5bpm)疗程期间心率均增加。所有缺氧疗程期间动脉血压均升高,尽管仅在IH中,从S1到S3基线常氧收缩压降低(-8±11mmHg)。两种缺氧干预在S3而非S1期间肌肉氧合显著降低(S3:SH -6±5%,IH -3±4%);前额叶氧合在S1和S3降低,且SH比IH降低幅度更大(-13±3%对-6±6%)。心率变异性指标表明,SH比IH交感神经活动增加显著更大(SH中SDNN、PNN50和RMSSD值更低)。从S1到S3,SH中观察到心率变异性进一步降低(SDNN、PNN50和RMSSD降低),而IH中心率变异性增加(SDNN和RMSSD增加)。这些结果表明,在短期SH与IH预处理干预期间,心率变异性、血压和组织氧合变化存在显著差异。心率变异性可能为这种干预诱导的早期适应提供有用信息。