Journel Ito, Andrécy Lesly L, Metellus Dudley, Pierre Jean S, Faublas Rose Murka, Juin Stanley, Dismer Amber M, Fitter David L, Neptune Daniel, Laraque Marie José, Corvil Salomon, Pierre Manise, Buteau Josiane, Lafontant Donald, Patel Roopal, Lemoine Jean Frantz, Lowrance David W, Charles Macarthur, Boncy Jacques, Adrien Paul
MMWR Morb Mortal Wkly Rep. 2017 Feb 17;66(6):172-176. doi: 10.15585/mmwr.mm6606a4.
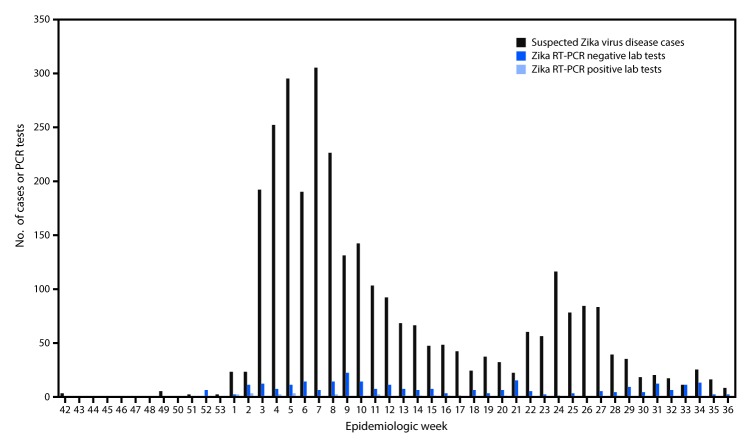
Zika virus disease is caused by infection with a flavivirus with broad geographic distribution and is most frequently transmitted by the bite of an infected mosquito. The disease was first identified in the World Health Organization's Region of the Americas in 2015 and was followed by a surge in reported cases of congenital microcephaly in Brazil; Zika virus disease rapidly spread to the rest of the region and the Caribbean (1), including Haiti. Infection with the virus is associated with adverse fetal outcomes (1) and rare neurologic complications in adults. The magnitude of public health issues associated with Zika virus led the World Health Organization to declare the Zika virus outbreak a Public Health Emergency of International Concern on February 1, 2016 (2). Because many persons with mild Zika virus disease are asymptomatic and might not seek care, it is difficult to estimate the actual incidence of Zika virus infection. During October 12, 2015-September 10, 2016, the Haitian Ministry of Public Health and Population (Ministère de la Santé Publique et de la Population [MSPP]) detected 3,036 suspected cases of Zika virus infection in the general population, 22 suspected cases of Zika virus disease among pregnant women, 13 suspected cases of Guillain-Barré syndrome (GBS), and 29 suspected cases of Zika-associated congenital microcephaly. Nineteen (0.6%) patients with suspected Zika virus disease, residing in Ouest (10 patients), Artibonite (six), and Centre (three) administrative departments,* have been confirmed by laboratory testing, including two among pregnant women and 17 in the general population. Ongoing laboratory-enhanced surveillance to monitor Zika virus disease in Haiti is important to understanding the outbreak and ensuring effective response activities.
寨卡病毒病由一种广泛分布于世界各地的黄病毒感染所致,主要通过受感染蚊子叮咬传播。该疾病于2015年在世界卫生组织美洲区域首次被发现,随后巴西报告的先天性小头畸形病例激增;寨卡病毒病迅速蔓延至该区域其他地区及加勒比地区(包括海地)(1)。感染该病毒与不良胎儿结局(1)及成人罕见的神经并发症有关。与寨卡病毒相关的公共卫生问题的严重程度促使世界卫生组织于2016年2月1日宣布寨卡病毒疫情为国际关注的突发公共卫生事件(2)。由于许多寨卡病毒轻症患者无症状且可能未寻求治疗,因此难以估计寨卡病毒感染的实际发病率。在2015年10月12日至2016年9月10日期间,海地公共卫生和人口部(Ministère de la Santé Publique et de la Population [MSPP])在普通人群中检测到3036例寨卡病毒感染疑似病例,孕妇中有22例寨卡病毒病疑似病例,13例吉兰-巴雷综合征(GBS)疑似病例,以及29例寨卡病毒相关先天性小头畸形疑似病例。居住在西部(10例)、阿蒂博尼特(6例)和中部(3例)行政区*的19例(0.6%)寨卡病毒病疑似患者经实验室检测确诊,其中包括2例孕妇和1例普通人群。在海地持续开展实验室强化监测以监测寨卡病毒病,对于了解疫情及确保有效应对措施至关重要。