Walker Rachael C, Howard Kirsten, Morton Rachael L
School of Public Health, Sydney Medical School, University of Sydney, Sydney, Australia; Hawke's Bay District Health Board, Hastings, New Zealand.
School of Public Health, Sydney Medical School, University of Sydney, Sydney, Australia.
Clinicoecon Outcomes Res. 2017 Feb 16;9:149-161. doi: 10.2147/CEOR.S69340. eCollection 2017.
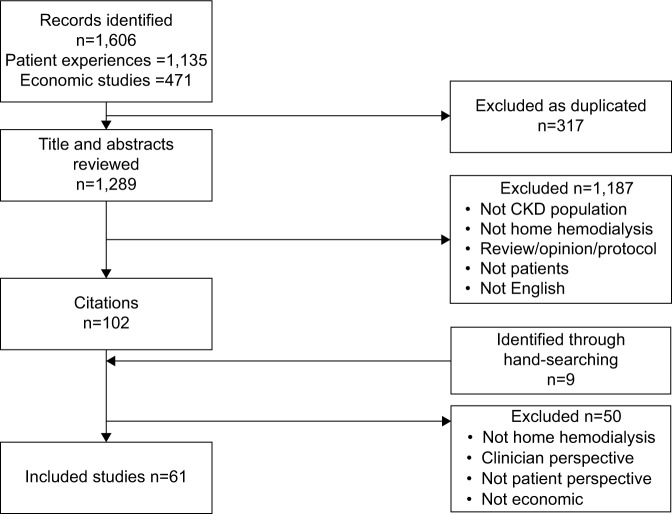
Internationally, the number of patients requiring treatment for end-stage kidney disease (ESKD) continues to increase, placing substantial burden on health systems and patients. Home hemodialysis (HD) has fluctuated in its popularity, and the rates of home HD vary considerably between and within countries although there is evidence suggesting a number of clinical, survival, economic, and quality of life (QoL) advantages associated with this treatment. International guidelines encourage shared decision making between patients and clinicians for the type of dialysis, with an emphasis on a treatment that aligned to the patients' lifestyle. This is a comprehensive literature review of patient-centered and economic impacts of home HD with the studies published between January 2000 and July 2016. Data from the primary studies representing both efficiency and equity of home HD were presented as a narrative synthesis under the following topics: advantages to patients, barriers to patients, economic factors influencing patients, cost-effectiveness of home HD, and inequities in home HD delivery. There were a number of advantages for patients on home HD including improved survival and QoL and flexibility and potential for employment, compared to hospital HD. Similarly, there were several barriers to patients preferring or maintaining home HD, and the strategies to overcome these barriers were frequently reported. Good evidence reported that indigenous, low-income, and other socially disadvantaged individuals had reduced access to home HD compared to other forms of dialysis and that this situation compounds already-poor health outcomes on renal replacement therapy. Government policies that minimize barriers to home HD include reimbursement for dialysis-related out-of-pocket costs and employment-retention interventions for home HD patients and their family members. This review argues that home HD is a cost-effective treatment, and increasing the proportion of patients on this form of dialysis compared to hospital HD will result in a more equitable distribution of good health outcomes for individuals with ESKD.
在国际上,需要接受终末期肾病(ESKD)治疗的患者数量持续增加,给卫生系统和患者带来了沉重负担。家庭血液透析(HD)的普及程度有所波动,不同国家之间以及国家内部的家庭血液透析率差异很大,尽管有证据表明这种治疗方式在临床、生存、经济和生活质量(QoL)方面具有诸多优势。国际指南鼓励患者和临床医生就透析类型共同做出决策,重点是选择一种与患者生活方式相适应的治疗方法。这是一项对2000年1月至2016年7月期间发表的关于家庭血液透析以患者为中心的影响和经济影响的综合文献综述。代表家庭血液透析效率和公平性的主要研究数据在以下主题下以叙述性综合的形式呈现:对患者的优势、患者面临的障碍、影响患者的经济因素、家庭血液透析的成本效益以及家庭血液透析服务提供中的不公平现象。与医院血液透析相比,接受家庭血液透析的患者有许多优势,包括生存率提高、生活质量改善、灵活性以及就业潜力。同样,患者选择或维持家庭血液透析也存在一些障碍,并且经常报道克服这些障碍的策略。有充分证据表明,与其他形式的透析相比,原住民、低收入和其他社会弱势群体接受家庭血液透析的机会减少,而且这种情况会使肾替代治疗本就不佳的健康结果更加恶化。将家庭血液透析相关自付费用纳入报销范围以及对家庭血液透析患者及其家庭成员实施就业保留干预等政府政策,可最大限度地减少家庭血液透析的障碍。本综述认为,家庭血液透析是一种具有成本效益的治疗方法,与医院血液透析相比,增加接受这种透析形式的患者比例将使ESKD患者更公平地获得良好的健康结果。