Parseghian Christine M, Parikh Nila U, Wu Ji Yuan, Jiang Zhi-Qin, Henderson Laura, Tian Feng, Pastor Brice, Ychou Marc, Raghav Kanwal, Dasari Arvind, Fogelman David R, Katsiampoura Anastasia D, Menter David G, Wolff Robert A, Eng Cathy, Overman Michael J, Thierry Alain R, Gallick Gary E, Kopetz Scott
Department of Gastrointestinal Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas.
IRCM, Institut de Recherche en Cancérologie de Montpellier, Montpellier, France.
Clin Cancer Res. 2017 Aug 1;23(15):4146-4154. doi: 10.1158/1078-0432.CCR-16-3138. Epub 2017 Mar 9.
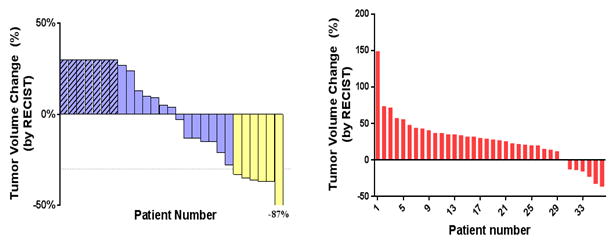
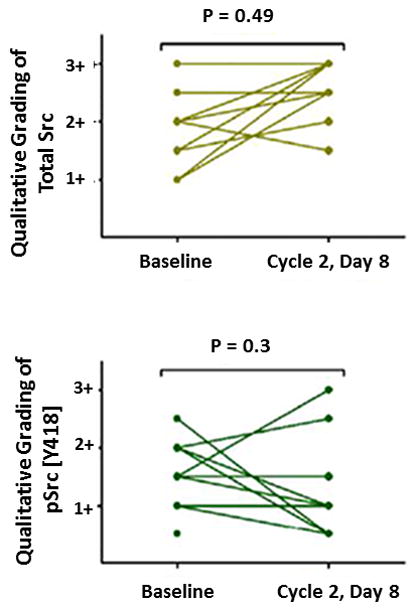
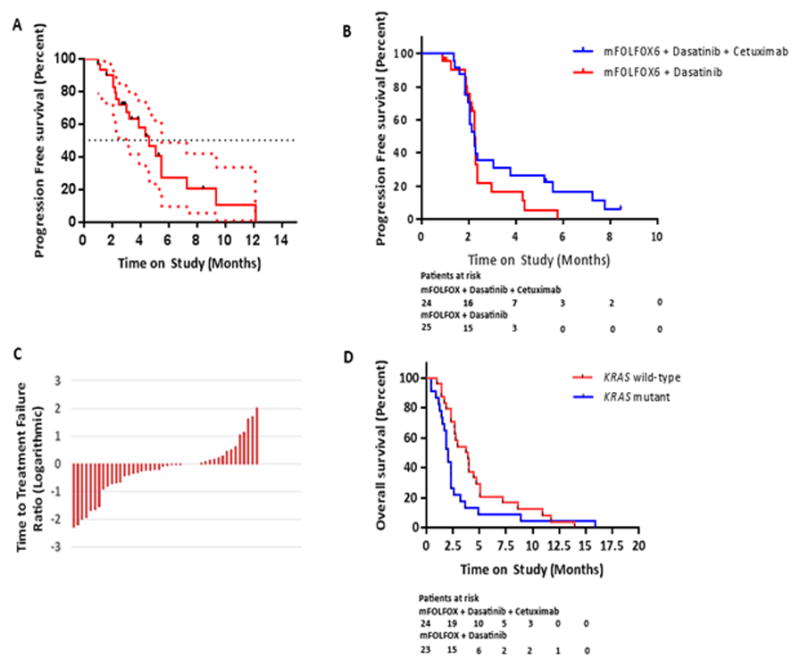
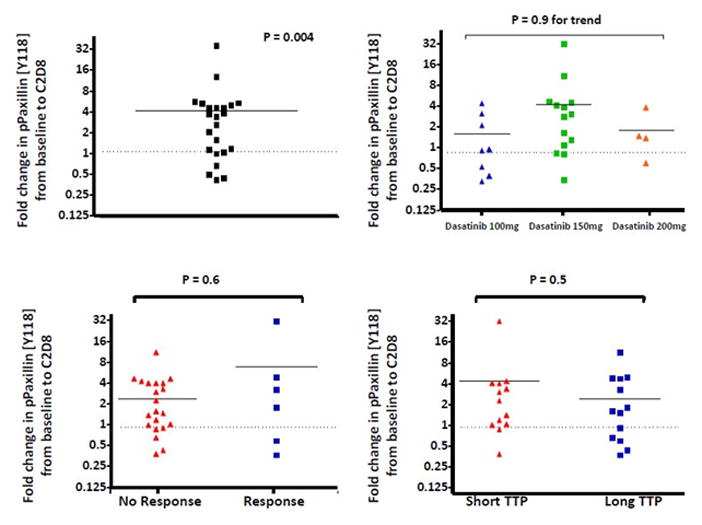
Aberrant activation of the intracellular tyrosine kinase Src has been implicated as a mechanism of acquired chemotherapy resistance in metastatic colorectal cancer (mCRC). Here, the oral tyrosine kinase Src inhibitor, dasatinib, was investigated in combination with FOLFOX and cetuximab. We performed a phase IB/II study of 77 patients with previously treated mCRC. Primary objectives were to determine the maximum tolerated dose, dose-limiting toxicities (DLT), pharmacodynamics, and efficacy. Using a 3 + 3 design, patients received FOLFOX6 with cetuximab and escalating doses of dasatinib (100, 150, 200 mg daily), followed by a 12-patient expansion cohort at 150 mg. Phase II studies evaluated FOLFOX plus dasatinib 100 mg in c12/13 patients or in combination with cetuximab if c12/13 FAK and paxillin were utilized as surrogate blood biomarkers of Src inhibition, and paired biopsies of liver metastases were obtained in patients in the expansion cohort. In phase IB, the DLTs were grade 3/4 fatigue (20%) and neutropenia (23%). In phase II, grade 3/4 fatigue (23%) and pleural effusions (11%) were present. Response rates were 20% (6 of 30) in the phase IB escalation and expansion cohort and 13% (3 of 24) and 0% (0 of 23) in the c12/13 and mutant cohorts of phase II, respectively. Median progression-free survival was 4.6, 2.3, and 2.3 months, respectively. There was no evidence of Src inhibition based on surrogate blood biomarkers or paired tumor biopsies. The combination of dasatinib plus FOLFOX with or without cetuximab showed only modest clinical activity in refractory colorectal cancer. This appears to be primarily due to a failure to fully inhibit Src at the achievable doses of dasatinib. The combination of dasatinib plus FOLFOX with or without cetuximab did not show meaningful clinical activity in refractory colorectal cancer due to failure to fully inhibit Src. .
细胞内酪氨酸激酶Src的异常激活被认为是转移性结直肠癌(mCRC)获得性化疗耐药的一种机制。在此,对口服酪氨酸激酶Src抑制剂达沙替尼联合FOLFOX和西妥昔单抗进行了研究。我们对77例先前接受过治疗的mCRC患者进行了一项1B/II期研究。主要目的是确定最大耐受剂量、剂量限制性毒性(DLT)、药效学和疗效。采用3+3设计,患者接受FOLFOX6联合西妥昔单抗以及递增剂量的达沙替尼(每日100、150、200mg),随后在150mg剂量组有一个12例患者的扩展队列。II期研究评估了FOLFOX联合100mg达沙替尼用于12/13例患者,或在12/13例FAK和桩蛋白用作Src抑制的替代血液生物标志物时联合西妥昔单抗,并在扩展队列的患者中获取肝转移灶的配对活检样本。在1B期,DLT为3/4级疲劳(20%)和中性粒细胞减少(23%)。在II期,出现了3/4级疲劳(23%)和胸腔积液(11%)。1B期剂量递增和扩展队列的缓解率为20%(30例中的6例),II期的12/13例和突变队列的缓解率分别为13%(24例中的3例)和0%(23例中的0例)。无进展生存期的中位数分别为4.6、2.3和2.3个月。基于替代血液生物标志物或配对肿瘤活检,没有证据表明Src受到抑制。达沙替尼联合FOLFOX加或不加西妥昔单抗在难治性结直肠癌中仅显示出适度的临床活性。这似乎主要是由于在可达到的达沙替尼剂量下未能完全抑制Src。达沙替尼联合FOLFOX加或不加西妥昔单抗在难治性结直肠癌中未显示出有意义的临床活性,原因是未能完全抑制Src。