Chen Wanqing, Zheng Rongshou, Zhang Siwei, Zeng Hongmei, Zuo Tingting, Xia Changfa, Yang Zhixun, He Jie
National Central Cancer Registry, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China.
Chin J Cancer Res. 2017 Feb;29(1):1-10. doi: 10.21147/j.issn.1000-9604.2017.01.01.
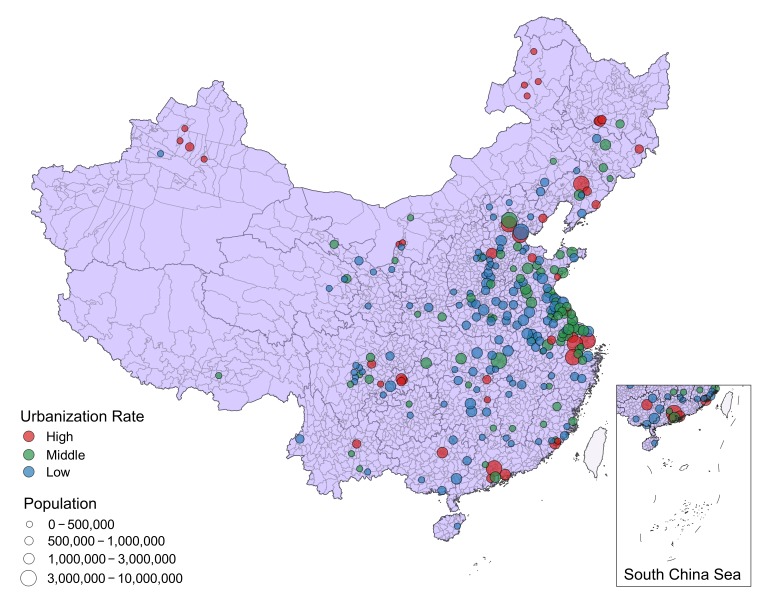
To explore the cancer patterns in areas with different urbanization rates (URR) in China with data from 255 population-based cancer registries in 2013, collected by the National Central Cancer Registry (NCCR).
There were 347 cancer registries submitted cancer incidence and deaths occurred in 2013 to NCCR. All those data were checked and evaluated based on the NCCR criteria of data quality, and qualified data from 255 registries were used for this analysis. According to the proportion of non-agricultural population, we divided cities/counties into 3 levels: high level, with URR equal to 70% and higher; median level, with URR between 30% and 70%; and low level, with URR equal to 30% and less. Cancer incidences and mortalities were calculated, stratified by gender and age groups in different areas. The national population of Fifth Census in 2000 and Segi's population were applied for age-standardized rates.
Qualified 255 cancer registries covered 226,494,490 populations. The percentage of cases morphologically verified (MV%) and death certificate-only cases (DCO%) were 68.04% and 1.74%, respectively, and the mortality to incidence rate ratio (M/I) was 0.62. A total of 644,487 new cancer cases and 399,275 cancer deaths from the 255 cancer registries were submitted to NCCR in 2013. The incidence rate was 284.55/100,000 (314.06/100,000 in males, 254.19/100,000 in females), and the age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 190.10/100,000 and 186.24/100,000 with the cumulative incidence rate (0-74 age years old) of 21.60%. The cancer mortality was 176.28/100,000 (219.03/100,000 in males, 132.30/100,000 in females), and the age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 110.91/100,000 and 109.92/100,000, and the cumulative mortality rate (0-74 age years old) was 12.43%. Low urbanization areas were high in crude cancer incidence and mortality rates, middle urbanization areas came next to it followed by high urbanization areas. After adjusted by age, there was a U-shaped association between age-standardized incidence (ASIRC and ASIRW) and the urbanized ratio with the middle urbanization areas having the lowest ASIRC and ASIRW. Unlike with the age-standardized incidence, the sort order of age-standardized mortality (ASMRC and ASMRW) among three urbanization areas was reversed completely from the crude mortality. Lung cancer was the most common cancer in all areas of 255 cancer registries, followed by stomach cancer, liver cancer, colorectal cancer and esophageal cancer with new cases of 130,700, 76,200, 63,800, 60,900 and 50,200 respectively. Lung cancer was also the leading cause of cancer death in all areas of 255 cancer registries for both males and females with the number of deaths of 72,200 and 34,100, respectively. Other cancer types with high mortality in males were liver cancer, stomach cancer, esophageal cancer and colorectal cancer. In females, stomach cancer was the second cause of cancer death, followed by liver cancer, colorectal cancer and breast cancer.
Along with the development of socioeconomics associated with urbanization, as well as the aging population, the incidence and mortality keep increasing in China. Cancer burden and patterns are different in each urbanization level. Cancer control strategies should be implemented referring to local urbanization status.
利用国家癌症中心(NCCR)收集的2013年来自255个基于人群的癌症登记处的数据,探讨中国不同城市化率地区的癌症模式。
共有347个癌症登记处向NCCR提交了2013年发生的癌症发病率和死亡数据。所有这些数据均根据NCCR的数据质量标准进行检查和评估,并使用来自255个登记处的合格数据进行本分析。根据非农业人口比例,将市/县分为3个级别:高城市化率地区,城市化率等于或高于70%;中等城市化率地区,城市化率在30%至70%之间;低城市化率地区,城市化率等于或低于30%。计算不同地区按性别和年龄组分层的癌症发病率和死亡率。采用2000年第五次全国人口普查的全国人口数据和Segi人口数据计算年龄标准化率。
255个合格癌症登记处覆盖了226494490人。形态学确诊病例百分比(MV%)和仅死亡证明病例百分比(DCO%)分别为68.04%和1.74%,死亡率与发病率之比(M/I)为0.62。2013年,255个癌症登记处共向NCCR提交了644487例新发癌症病例和399275例癌症死亡病例。发病率为284.55/10万(男性为314.06/10万,女性为254.19/10万),按中国标准人口计算的年龄标准化发病率(ASIRC)和按世界标准人口计算的年龄标准化发病率(ASIRW)分别为190.10/10万和186.24/10万,累积发病率(0至74岁)为21.60%。癌症死亡率为176.28/10万(男性为219.03/10万,女性为132.30/10万),按中国标准人口计算的年龄标准化死亡率(ASMRC)和按世界标准人口计算的年龄标准化死亡率(ASMRW)分别为110.91/10万和109.92/10万,累积死亡率(0至74岁)为12.43%。低城市化地区的癌症粗发病率和死亡率较高,中等城市化地区次之,高城市化地区最低。按年龄调整后,年龄标准化发病率(ASIRC和ASIRW)与城市化率呈U形关联,中等城市化地区的ASIRC和ASIRW最低。与年龄标准化发病率不同,三个城市化地区年龄标准化死亡率(ASMRC和ASMRW)的排序与粗死亡率完全相反。肺癌是255个癌症登记处所有地区最常见的癌症,其次是胃癌、肝癌、结直肠癌和食管癌,新发病例分别为130700例、76200例、63800例、60900例和50200例。肺癌也是255个癌症登记处所有地区男性和女性癌症死亡的主要原因,死亡人数分别为72200例和34100例。男性其他高死亡率癌症类型为肝癌、胃癌、食管癌和结直肠癌。在女性中,胃癌是癌症死亡的第二大原因,其次是肝癌、结直肠癌和乳腺癌。
随着与城市化相关的社会经济发展以及人口老龄化,中国的癌症发病率和死亡率持续上升。不同城市化水平的癌症负担和模式各不相同。应参照当地城市化状况实施癌症控制策略。