Emory University School of Medicine, Atlanta, GA.
Graduate School of Public Health, University of Pittsburgh, PA.
J Am Heart Assoc. 2017 Jul 3;6(7):e003587. doi: 10.1161/JAHA.116.003587.
In a previous study, we found that a biomarker risk score (BRS) comprised of C-reactive protein, fibrin-degradation products, and heat shock protein-70 predicts risk of myocardial infarction and death in coronary artery disease patients. We sought to: (1) validate the BRS in the independent BARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes) cohort, (2) investigate whether 1 year of intensive medical therapy is associated with improved BRS, and (3) elucidate whether an altered BRS parallels altered risk.
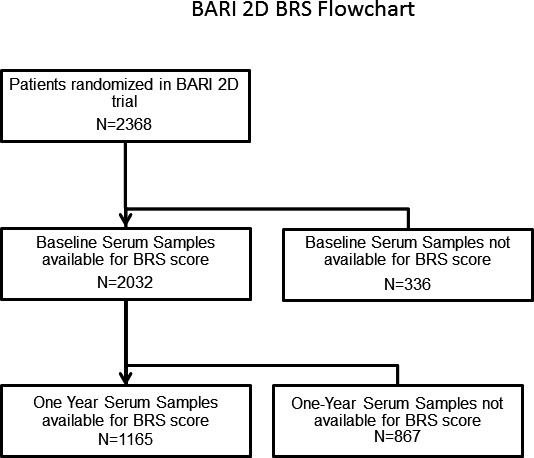
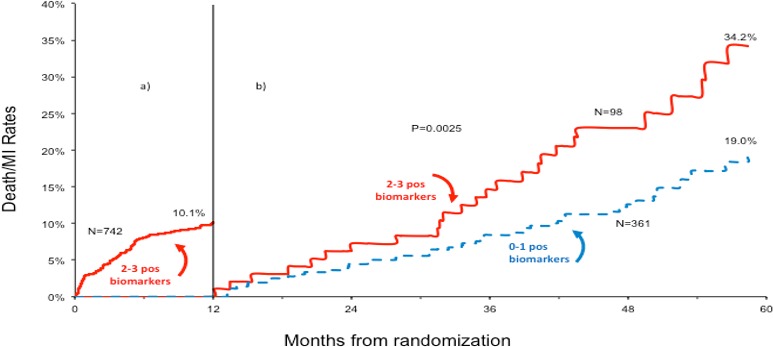
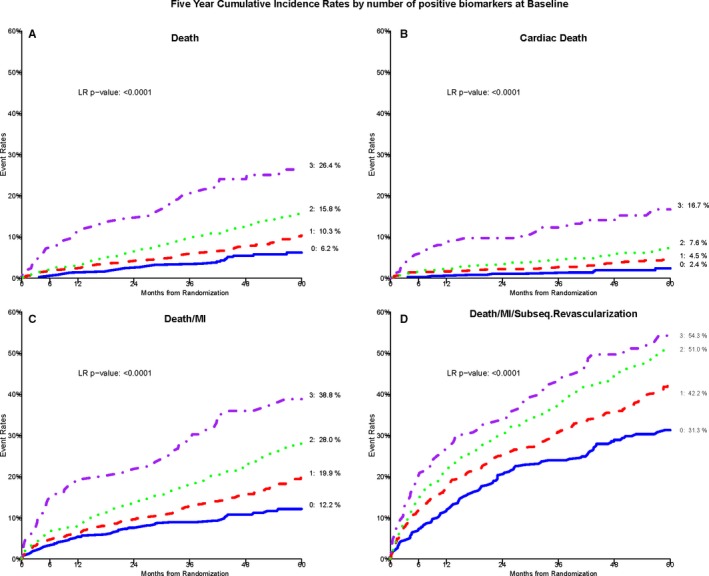
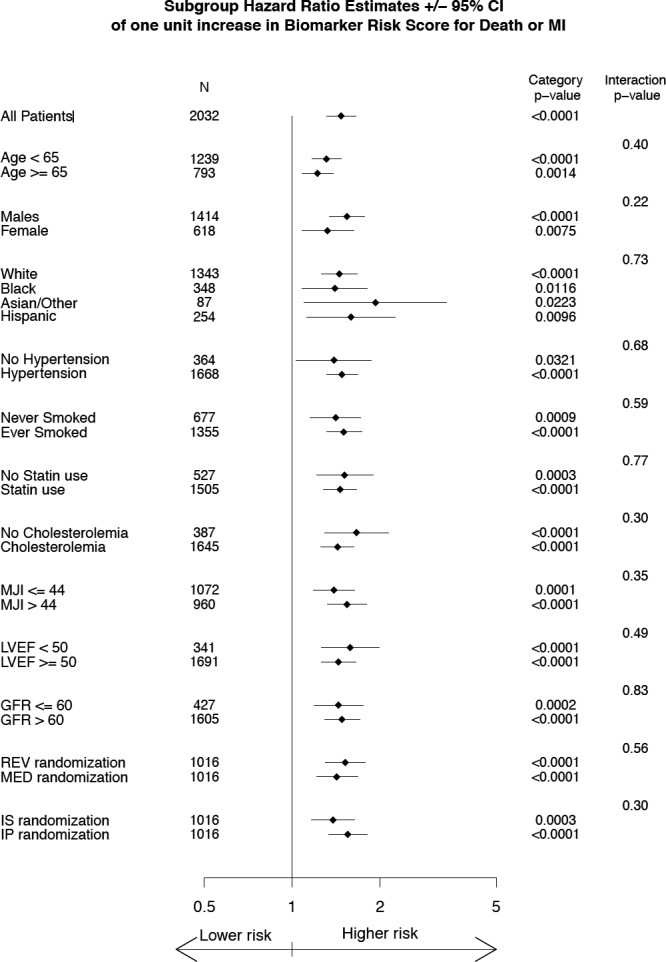
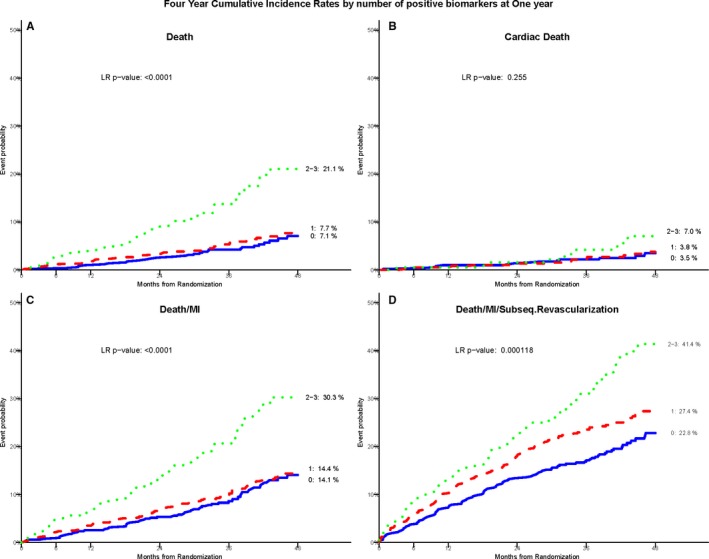
Two thousand thirty-two subjects with coronary artery disease were followed for 5.3±1.1 years for cardiovascular events. Biomarkers were measured at baseline and retested in 1304 subjects at 1 year. BRS was determined as the biomarker number above previously defined cut-off values (C-reactive protein >3 mg/L, heat shock protein-70 >0.313 ng/mL, and fibrin-degradation products >1 μg/mL). After adjustment for covariates, those with a BRS of 3 had a 4-fold increased risk of all-cause death and a 6.8-fold increased risk of cardiac death compared with those with a BRS of 0 (95% CI, 2.9-16.0; <0.0001). All individual biomarkers decreased by 1 year, with ≈80% of patients decreasing their BRS. BRS recalibrated at 1 year also predicted risk. Those with 1-year BRS of 2 to 3 had a 4-year mortality rate of 21.1% versus 7.4% for those with BRS of 0 to 1 (<0.0001).
Our results validate the ability of the BRS to identify coronary artery disease patients at very high near-term risk of myocardial infarction/death. After 1 year of intensive medical therapy, the BRS decreased significantly, and the reclassified BRS continued to track with risk. Our results suggest that repeated BRS measurements might be used to assess risk and recalibrate therapy.
在之前的一项研究中,我们发现由 C 反应蛋白、纤维蛋白降解产物和热休克蛋白 70 组成的生物标志物风险评分(BRS)可预测冠心病患者发生心肌梗死和死亡的风险。我们试图:(1)在独立的 BARI 2D(冠状动脉旁路移植术血管成形术再血管化调查 2 型糖尿病)队列中验证 BRS;(2)研究强化药物治疗 1 年是否与 BRS 的改善相关;(3)阐明 BRS 的变化是否与风险的变化平行。
2032 例冠心病患者随访 5.3±1.1 年发生心血管事件。在 1304 例患者中,基线时测量了生物标志物,并在 1 年时进行了复测。BRS 确定为先前定义的截断值(C 反应蛋白>3mg/L、热休克蛋白 70>0.313ng/mL 和纤维蛋白降解产物>1μg/mL)以上的生物标志物数量。经协变量调整后,BRS 为 3 的患者全因死亡风险增加 4 倍,心脏死亡风险增加 6.8 倍,而 BRS 为 0 的患者则增加 4 倍(95%CI,2.9-16.0;<0.0001)。所有单个生物标志物在 1 年内均下降,约 80%的患者降低了 BRS。1 年后重新校准的 BRS 也可预测风险。BRS 为 2 至 3 的患者在 4 年内的死亡率为 21.1%,而 BRS 为 0 至 1 的患者死亡率为 7.4%(<0.0001)。
我们的结果验证了 BRS 识别近期发生心肌梗死/死亡风险极高的冠心病患者的能力。强化药物治疗 1 年后,BRS 显著下降,重新分类的 BRS 继续跟踪风险。我们的结果表明,重复测量 BRS 可能用于评估风险和重新调整治疗。