Chang Jer-Hwa, Wu Chia-Che, Yuan Kevin Sheng-Po, Wu Alexander T H, Wu Szu-Yuan
Division of Pulmonary Medicine, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan.
School of Respiratory Therapy, College of Medicine, Taipei Medical University, Taipei, Taiwan.
Oncotarget. 2017 Mar 17;8(33):55600-55612. doi: 10.18632/oncotarget.16340. eCollection 2017 Aug 15.
For locoregionally recurrent head and neck squamous cell carcinoma (HNSCC), appropriate therapeutic decisions remain unclear. We examined the treatment outcomes of a national cohort to determine suitable treatments for and prognostic factors in patients with locoregionally recurrent HNSCCs at different stages and sites.
We analyzed data of >20-year-old patients with HNSCC at American Joint Committee on Cancer clinical stages I-IV without metastasis from Taiwan National Health Insurance and cancer registry databases. The index date was the date of recurrent HNSCC diagnosis. Recurrent HNSCC was defined as the annotation of locoregional recurrence with tissue proof in cancer registry databases. The enrolled patients were categorized into three groups: Group 1 comprised those undergoing chemotherapy (CT) alone; Group 2 comprised those receiving reirradiation (re-RT) alone (total radiation dose ≥ 60 Gy through intensity modulation radiation therapy [IMRT]); Group 3 comprised those receiving concurrent chemoradiotherapy (CCRT) alone (irradiation total dose ≥60 Gy through IMRT); and Group 4 comprised those receiving salvage surgery with or without RT or CT.
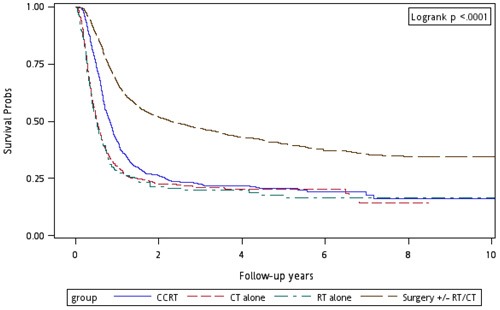
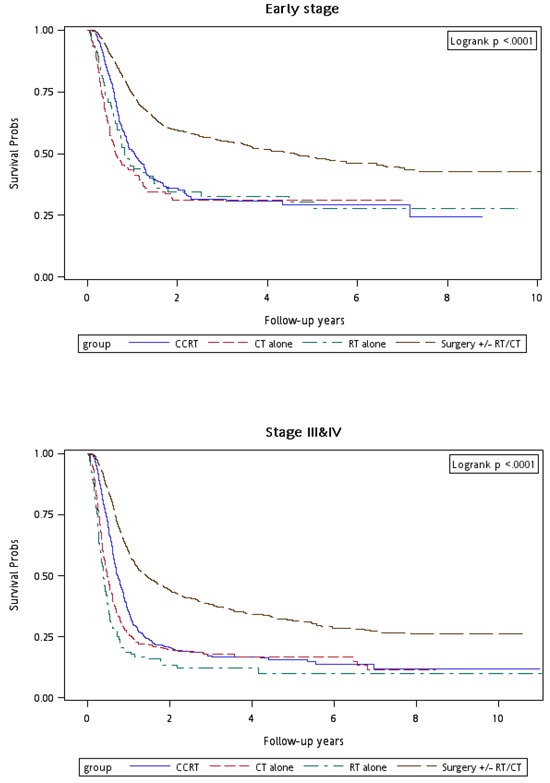
We enrolled 4,839 and 28,664 HNSCC patients with and without locoregional recurrence, respectively (median follow-up, 3.25 years). Locoregional recurrence rate and incidence were 14.44% and 40.73 per 1,000 person-years, respectively. Age ≥ 65 years, Charlson comorbidity index (CCI) score > 6, advanced clinical stage at first diagnosis, and recurrence-free interval < 1 year were significant independent prognostic risk factors for overall survival as per univariate and multivariate Cox regression analyses. After adjusting for age, sex, CCI scores, clinical stage at first diagnosis, and recurrence-free interval, adjusted hazard ratios (aHRs; 95% confidence intervals [CIs]) for overall mortality in recurrent clinical stages I and II were 0.63 (0.45-0.89, = 0.009), 0.65 (0.52-0.83, < 0.001), and 0.32 (0.26-0.40, < 0.001) in Groups 2, 3, and 4, respectively, whereas they were 1.23 (0.99-1.52, = 0.062), 0.69 (0.60-0.79, < 0.001), and 0.39 (0.34-0.44, < 0.001) for Groups 2, 3, and 4, respectively, for overall mortality in recurrent clinical stage III and IV.
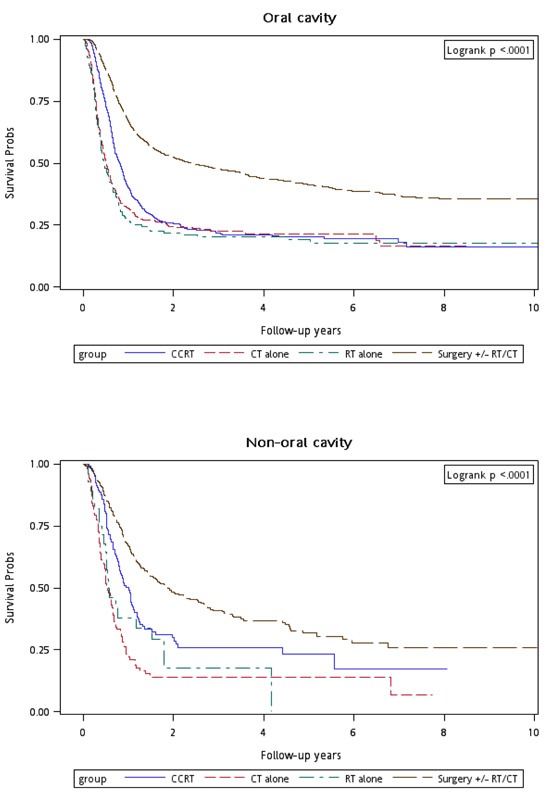
Age, CCI score, clinical stage at first diagnosis, and recurrence-free interval are significant independent prognostic factors for overall survival of recurrent HNSCC patients. Regardless of recurrence stage or site, salvage surgery is the recommended first recurrent HNSCC treatment choice. Re-RT alone and CCRT are more suitable for inoperable recurrent early-stage oral and nonoral cavity recurrent HNSCCs, respectively.
对于局部区域复发的头颈部鳞状细胞癌(HNSCC),合适的治疗决策仍不明确。我们研究了一个全国队列的治疗结果,以确定不同分期和部位的局部区域复发HNSCC患者的合适治疗方法及预后因素。
我们分析了来自台湾国民健康保险和癌症登记数据库中年龄大于20岁、美国癌症联合委员会临床分期为I-IV期且无转移的HNSCC患者的数据。索引日期为复发性HNSCC的诊断日期。复发性HNSCC定义为癌症登记数据库中经组织证实的局部区域复发标注。入组患者分为三组:第1组为仅接受化疗(CT)的患者;第2组为仅接受再程放疗(re-RT)的患者(通过调强放射治疗[IMRT]的总辐射剂量≥60 Gy);第3组为仅接受同步放化疗(CCRT)的患者(通过IMRT的照射总剂量≥60 Gy);第4组为接受挽救性手术联合或不联合放疗或化疗的患者。
我们分别纳入了4839例有局部区域复发和28664例无局部区域复发的HNSCC患者(中位随访时间为3.25年)。局部区域复发率和发病率分别为14.44%和每1000人年40.73例。根据单因素和多因素Cox回归分析,年龄≥65岁、Charlson合并症指数(CCI)评分>6、首次诊断时临床分期较晚以及无复发生存期<1年是总生存的显著独立预后危险因素。在调整年龄、性别、CCI评分、首次诊断时的临床分期和无复发生存期后,复发性临床I期和II期患者的总死亡率调整后风险比(aHRs;95%置信区间[CIs])在第2组、第3组和第4组中分别为0.63(0.45 - 0.89,P = 0.009)、0.65(0.52 - 0.83,P < 0.001)和0.32(0.26 - 0.40,P < 0.001),而复发性临床III期和IV期患者的总死亡率调整后风险比在第2组、第3组和第4组中分别为1.23(0.99 - 1.52,P = 0.062)、0.69(0.60 - 0.79,P < 0.001)和0.39(0.34 - 0.44,P < 0.001)。
年龄、CCI评分、首次诊断时的临床分期和无复发生存期是复发性HNSCC患者总生存的显著独立预后因素。无论复发分期或部位如何,挽救性手术是推荐的复发性HNSCC的首选治疗方法。单纯再程放疗和同步放化疗分别更适用于无法手术的复发性早期口腔和非口腔复发性HNSCC。