Taklalsingh Nicholas, Falcone Franco, Velayudhan Vinodkumar
Department of Internal Medicine, State University of New York (SUNY) Downstate Medical Center, Brooklyn, NY, USA.
Department of Radiology, State University of New York (SUNY) Downstate Medical Center, Brooklyn, NY, USA.
Am J Case Rep. 2017 Sep 28;18:1039-1043. doi: 10.12659/ajcr.904648.
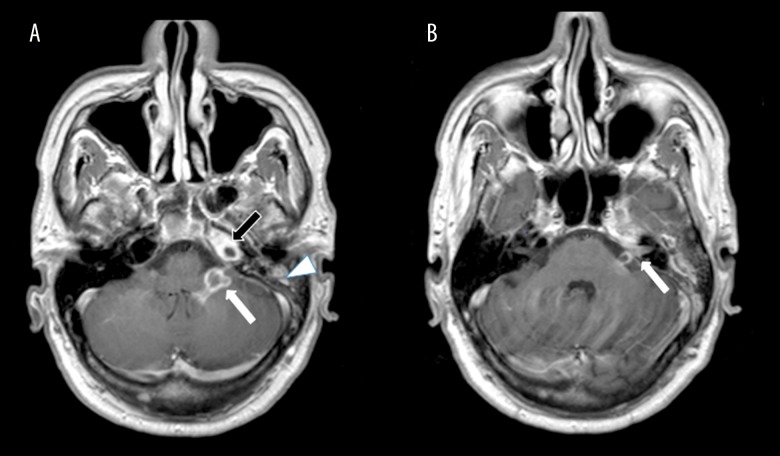
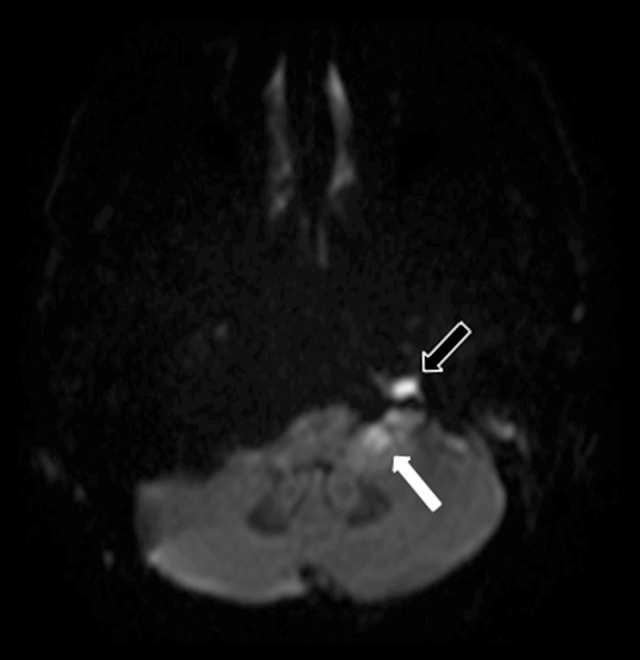
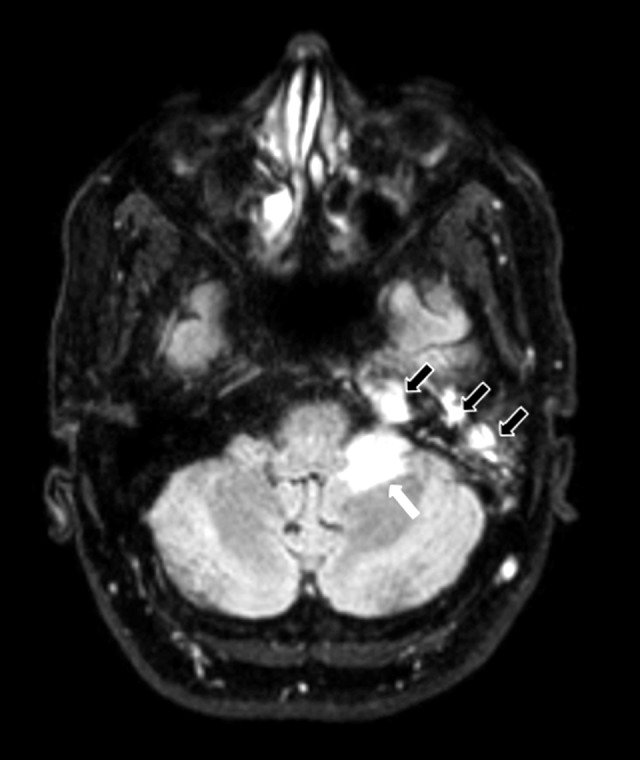
BACKGROUND Gradenigo's syndrome includes the triad of suppurative otitis media, ipsilateral sixth (abducens) cranial nerve palsy and facial pain in the distribution of the fifth (trigeminal) cranial nerve. Gradenigo's syndrome is rare, and the diagnosis is easily overlooked. This case is the first to report Gradenigo's syndrome presenting with meningitis on a background of chronic suppurative otitis media (CSOM) and petrous apicitis (apical petrositis). CASE REPORT A 58-year-old male African American presented with headaches and confusion. Magnetic resonance imaging (MRI) of the head showed petrous apicitis with mastoiditis and abscess formation in the cerebellomedullary cistern (cisterna magna). The case was complicated by the development of palsy of the fourth (trochlear) cranial nerve, fifth (trigeminal) cranial nerve, and sixth (abducens) cranial nerve, with radiological changes indicating infection involving the seventh (facial) cranial nerve, and eighth (vestibulocochlear) cranial nerve. Cerebrospinal fluid (CSF) culture results were positive for Klebsiella pneumoniae, sensitive to ceftriaxone. The patient improved with surgery that included a left mastoidectomy and debridement of the petrous apex, followed by a ten-week course of antibiotics. Follow-up MRI showed resolution of the infection. CONCLUSIONS This report is of an atypical case of Gradenigo's syndrome. It is important to recognize that the classical triad of Gradenigo's syndrome, suppurative otitis media, ipsilateral sixth (abducens) cranial nerve palsy and facial pain in the distribution of the fifth (trigeminal) cranial nerve, may also involve chronic suppurative otitis media (CSOM), which may lead to involvement of other cranial nerves, petrous apicitis (apical petrositis), and bacterial meningitis.
Gradenigo综合征包括化脓性中耳炎、同侧第六(展)脑神经麻痹以及第五(三叉)脑神经分布区域的面部疼痛三联征。Gradenigo综合征较为罕见,诊断容易被忽视。该病例是首例报道在慢性化脓性中耳炎(CSOM)和岩尖炎(岩尖骨炎)背景下出现脑膜炎表现的Gradenigo综合征。
一名58岁的非洲裔美国男性出现头痛和意识模糊。头部磁共振成像(MRI)显示岩尖炎伴乳突炎以及小脑延髓池(枕大池)脓肿形成。该病例并发第四(滑车)脑神经、第五(三叉)脑神经和第六(展)脑神经麻痹,影像学改变提示感染累及第七(面)脑神经和第八(前庭蜗)脑神经。脑脊液(CSF)培养结果显示肺炎克雷伯菌阳性,对头孢曲松敏感。患者通过包括左侧乳突切除术和岩尖清创术的手术治疗,随后接受为期十周的抗生素治疗后病情好转。随访MRI显示感染消退。
本报告为Gradenigo综合征的非典型病例。重要的是要认识到,Gradenigo综合征的经典三联征,即化脓性中耳炎、同侧第六(展)脑神经麻痹以及第五(三叉)脑神经分布区域的面部疼痛,也可能涉及慢性化脓性中耳炎(CSOM),这可能导致其他脑神经受累、岩尖炎(岩尖骨炎)和细菌性脑膜炎。