Institute of Infection, Immunity and Inflammation, College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK.
British Society for Cardiovascular Research, UK.
Heart. 2018 Mar;104(6):460-467. doi: 10.1136/heartjnl-2017-311447. Epub 2017 Oct 23.
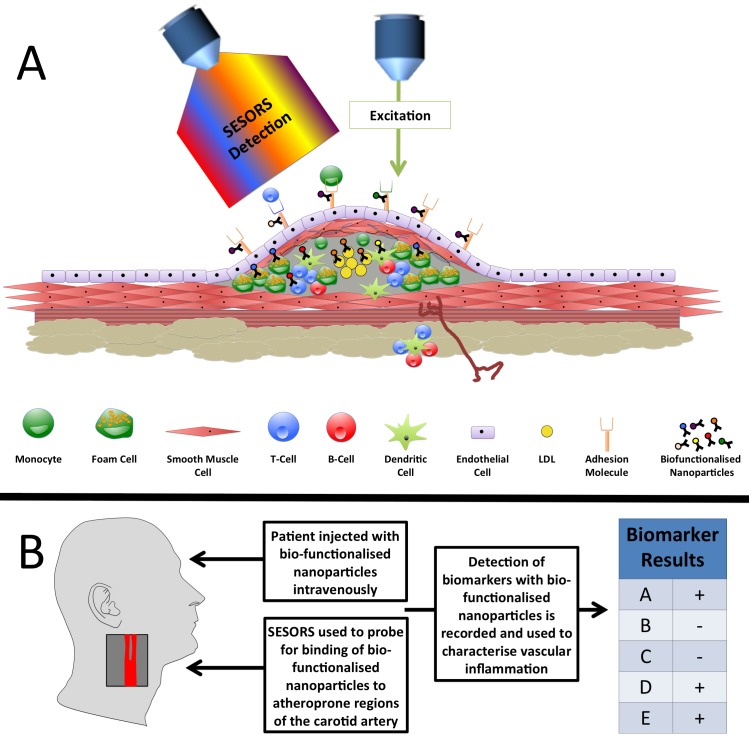
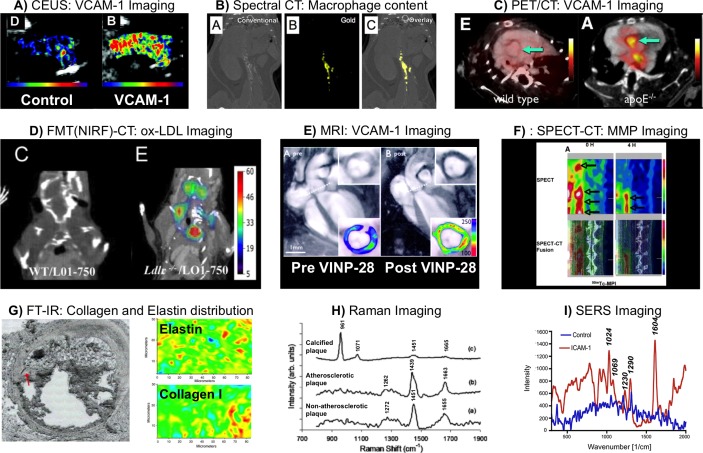
To accurately predict atherosclerotic plaque progression, a detailed phenotype of the lesion at the molecular level is required. Here, we assess the respective merits and limitations of molecular imaging tools. Clinical imaging includes contrast-enhanced ultrasound, an inexpensive and non-toxic technique but with poor sensitivity. CT benefits from high spatial resolution but poor sensitivity coupled with an increasing radiation burden that limits multiplexing. Despite high sensitivity, positron emission tomography and single-photon emission tomography have disadvantages when applied to multiplex molecular imaging due to poor spatial resolution, signal cross talk and increasing radiation dose. In contrast, MRI is non-toxic, displays good spatial resolution but poor sensitivity. Preclinical techniques include near-infrared fluorescence (NIRF), which provides good spatial resolution and sensitivity; however, multiplexing with NIRF is limited, due to photobleaching and spectral overlap. Fourier transform infrared spectroscopy and Raman spectroscopy are label-free techniques that detect molecules based on the vibrations of chemical bonds. Both techniques offer fast acquisition times with Raman showing superior spatial resolution. Raman signals are inherently weak; however, leading to the development of surface-enhanced Raman spectroscopy (SERS) that offers greatly increased sensitivity due to using metallic nanoparticles that can be functionalised with biomolecules targeted against plaque ligands while offering high multiplexing potential. This asset combined with high spatial resolution makes SERS an exciting prospect as a diagnostic tool. The ongoing refinements of SERS technologies such as deep tissue imaging and portable systems making SERS a realistic prospect for translation to the clinic.
为了准确预测动脉粥样硬化斑块的进展,需要在分子水平上对病变进行详细的表型分析。在这里,我们评估了分子成像工具的各自优缺点。临床成像包括对比增强超声,这是一种廉价且无毒的技术,但灵敏度较差。CT 具有较高的空间分辨率,但灵敏度较差,加上辐射负担增加,限制了其多重应用。尽管正电子发射断层扫描和单光子发射断层扫描具有较高的灵敏度,但由于空间分辨率差、信号串扰和辐射剂量增加,在应用于多重分子成像时存在缺点。相比之下,磁共振成像(MRI)无毒,具有良好的空间分辨率,但灵敏度较差。在临床前技术方面,近红外荧光(NIRF)提供了良好的空间分辨率和灵敏度;然而,由于光漂白和光谱重叠,NIRF 的多重应用受到限制。傅里叶变换红外光谱和拉曼光谱是基于化学键振动来检测分子的无标记技术。这两种技术都具有快速采集时间,拉曼光谱具有更高的空间分辨率。然而,拉曼信号较弱;因此,发展了表面增强拉曼光谱(SERS),由于使用可以与针对斑块配体的生物分子功能化的金属纳米粒子,SERS 具有极大提高的灵敏度,同时具有高多重应用潜力。这一优势结合高空间分辨率,使 SERS 成为一种令人兴奋的诊断工具前景。SERS 技术的不断改进,如深层组织成像和便携式系统,使 SERS 成为向临床转化的现实前景。