Department of Cardiology, Academic Medical Center, Room G4-230, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
Department of Radiology, Academic Medical Center, Meibergdreef 9, 1105 AZ, Amsterdam, the Netherlands.
Eur Heart J. 2017 Oct 21;38(40):3006-3013. doi: 10.1093/eurheartj/ehx318.
Mechanical chest compression (CC) during cardiopulmonary resuscitation (CPR) with AutoPulse or LUCAS devices has not improved survival from cardiac arrest. Cohort studies suggest risk of excess damage. We studied safety of mechanical CC and determined possible excess damage compared with manual CC.
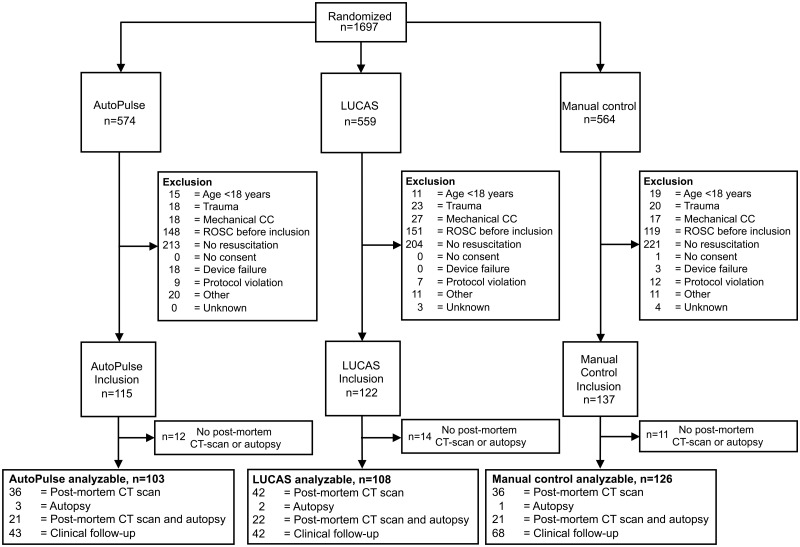
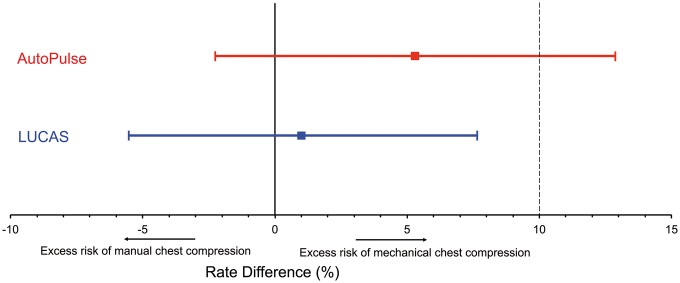
This is a randomized non-inferiority safety study. Randomization to AutoPulse, LUCAS, or manual CC with corrective depth and rate feedback was performed. We included patients with in-hospital cardiac arrest or with out-of-hospital cardiac arrest arriving with manual CPR at the emergency department. The primary outcome was serious or life-threatening visceral resuscitation-related damage, assessed blind by post-mortem computed tomography scan and/or autopsy or by clinical course until discharge. Non-inferiority hypothesis: mechanical CC compared with manual control does not increase the primary outcome by a risk difference of > 10% [upper 95% confidence interval (CI)]. We included 115 patients treated with AutoPulse, 122 with LUCAS, and 137 patients received manual CC. Safety outcome analysis was possible in 337 of 374 (90.1%) included patients. The primary outcome was observed in 12 of 103 AutoPulse patients (11.6%), 8 of 108 LUCAS patients (7.4%), and 8 of 126 controls (6.4%). Rate difference AutoPulse-control: +5.3% (95% CI - 2.2% to 12.8%), P = 0.15. Rate difference LUCAS-control +1.0% (95% CI - 5.5% to 7.6%), P = 0.75.
LUCAS does not cause significantly more serious or life-threatening visceral damage than manual CC. For AutoPulse, significantly more serious or life-threatening visceral damage than manual CC cannot be excluded.
心肺复苏期间使用 AutoPulse 或 LUCAS 装置进行机械胸外按压(CC)并未提高心搏骤停患者的存活率。队列研究表明存在过度损伤的风险。我们研究了机械 CC 的安全性,并确定了与手动 CC 相比可能存在的过度损伤。
这是一项随机非劣效性安全性研究。对 AutoPulse、LUCAS 或带有纠正深度和速率反馈的手动 CC 进行随机分组。我们纳入了院内心搏骤停或在急诊科接受手动心肺复苏的院外心搏骤停患者。主要结局为严重或危及生命的与复苏相关的内脏损伤,通过死后计算机断层扫描和/或尸检或直至出院的临床过程进行盲法评估。非劣效性假设:与手动对照相比,机械 CC 不会使主要结局的风险差异增加超过 10%[上限 95%置信区间(CI)]。我们纳入了 115 例 AutoPulse 治疗患者、122 例 LUCAS 治疗患者和 137 例接受手动 CC 治疗的患者。374 例纳入患者中有 337 例可进行安全性结局分析。主要结局在 103 例 AutoPulse 患者中的 12 例(11.6%)、108 例 LUCAS 患者中的 8 例(7.4%)和 126 例对照组患者中的 8 例(6.4%)中观察到。AutoPulse 与对照组的速率差异:+5.3%(95%CI-2.2%至 12.8%),P=0.15。LUCAS 与对照组的速率差异:+1.0%(95%CI-5.5%至 7.6%),P=0.75。
与手动 CC 相比,LUCAS 并未导致严重或危及生命的内脏损伤显著增加。对于 AutoPulse,不能排除其与手动 CC 相比严重或危及生命的内脏损伤显著增加的可能性。