Epstein Nancy E, Hollingsworth Renee D
NYU Winthrop Hospital, Mineola, New York, USA.
Surg Neurol Int. 2017 Oct 10;8:246. doi: 10.4103/sni.sni_276_17. eCollection 2017.
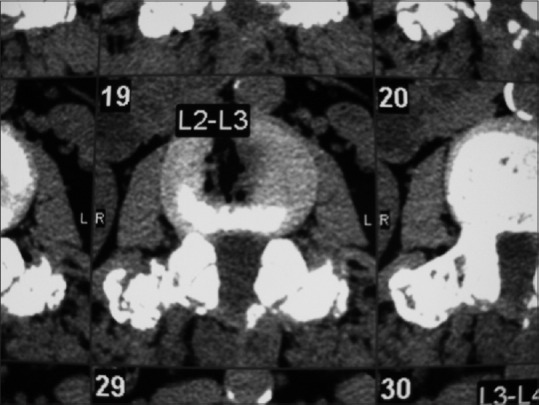
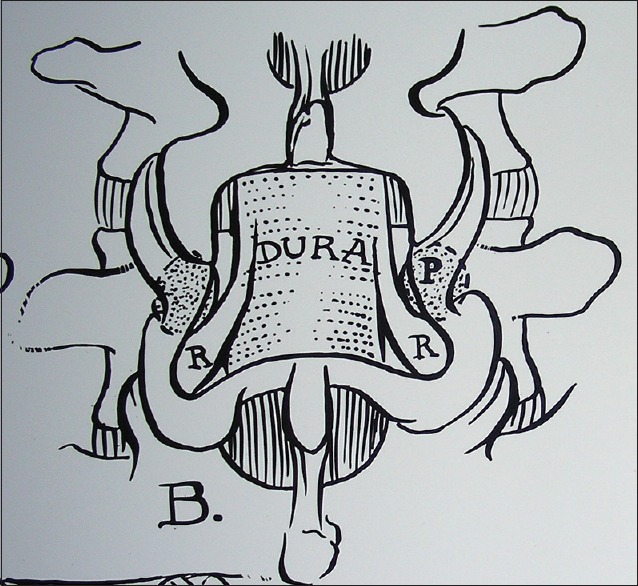
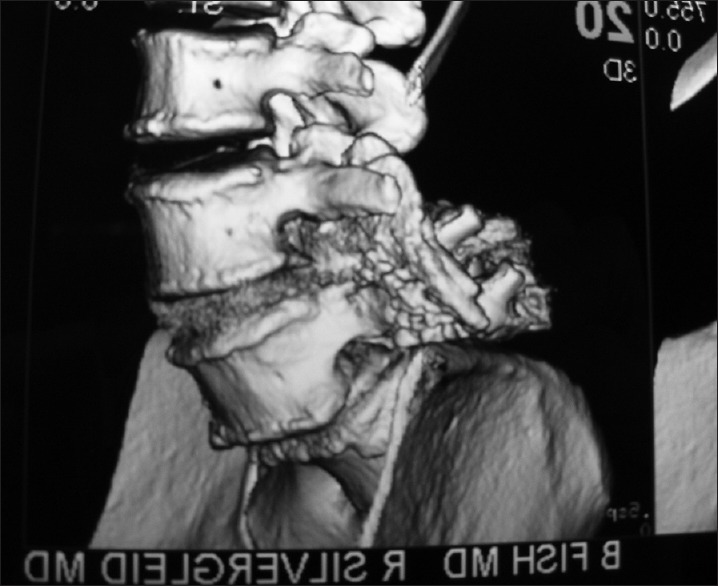
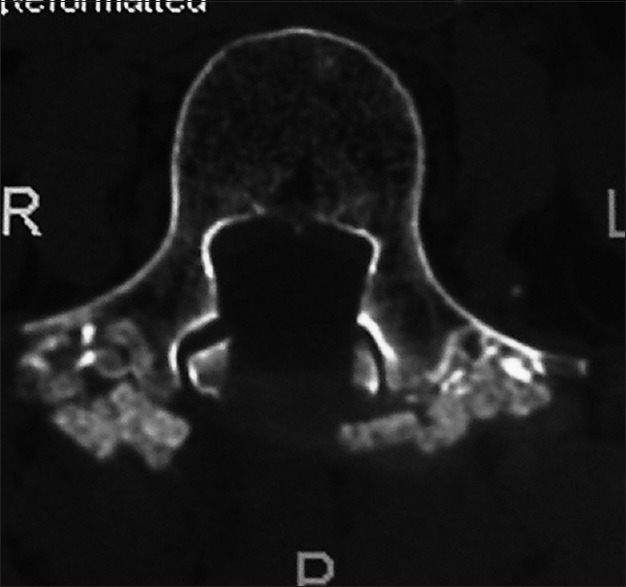
In the lumbar spine, degenerative spondylolisthesis or degenerative (not traumatic) slippage of one vertebral body over another is divided into 4 grades - grade I (25%), grade II (50%), grade III (75%), and grade IV (100%). Dynamic X-rays, magnetic resonance (MR), and computed tomography (CT) scans document the slip secondary to arthritic changes of the facet joint plus stenosis, ossification of the yellow ligament, disc herniations, and synovial cysts. MR best demonstrates soft tissue pathology whereas CT better delineates ossific/calcified disease.
Grade I degenerative spondylolisthesis, typically found at the L4-L5 level followed by L3-L4 and L5S1, is more common in females (ratio 2:1) over the age of 65. Symptoms include radiculopathy (root pain) and neurogenic claudication (e.g., pain with ambulation, requiring the patient to stop, rest, sit down). Symptoms/signs may include unilateral/bilateral radiculopathy and uni/multifocal motor, reflex, and sensory deficits in. Some may also present with a cauda equina syndrome (e.g., paraparesis/sphincter dysfunction).
Surgery for grade I-II spondylolisthesis may include laminectomy alone, laminectomy/noninstrumented fusion or with an instrumented fusion. Older patients with osteoporosis are more likely to have no fusion or a noninstrumented fusion. All fusions utilize autograft harvested from the laminectomy that may or may not be combined with a bone graft expander (to increase the fusion mass) combined with autogenous bone marrow aspirate. The fusion mass is placed over the transverse processes following decortication.
Patients with multilevel spinal stenosis and degenerative spondylolisthesis may require decompressive lumbar laminectomies alone or in combination with noninstrumented or instrumented fusions.
在腰椎,退行性椎体滑脱或一个椎体相对于另一个椎体的退行性(非创伤性)滑移分为4级——I级(25%)、II级(50%)、III级(75%)和IV级(100%)。动态X线、磁共振成像(MR)和计算机断层扫描(CT)可记录因小关节关节炎改变继发的滑移,以及椎管狭窄、黄韧带骨化、椎间盘突出和滑膜囊肿。MR能最佳地显示软组织病变,而CT能更好地描绘骨化/钙化性疾病。
I级退行性椎体滑脱通常见于L4-L5节段,其次是L3-L4和L5-S1节段,在65岁以上女性中更为常见(比例为2:1)。症状包括神经根病(根性疼痛)和神经源性间歇性跛行(如行走时疼痛,需患者停下、休息、坐下)。症状/体征可能包括单侧/双侧神经根病以及单灶/多灶性运动、反射和感觉障碍。有些人还可能出现马尾综合征(如轻截瘫/括约肌功能障碍)。
I-II级椎体滑脱的手术可能包括单纯椎板切除术、椎板切除术/非器械融合术或器械融合术。患有骨质疏松症的老年患者更可能不进行融合或采用非器械融合术。所有融合术均使用从椎板切除术中获取的自体骨移植,其可能与或不与骨移植扩张器(以增加融合块)及自体骨髓抽吸物联合使用。在进行去皮质处理后,将融合块置于横突上。
患有多节段椎管狭窄和退行性椎体滑脱的患者可能需要单独进行减压性腰椎椎板切除术,或与非器械或器械融合术联合进行。