Pu Ning, Gao Shanshan, Xu Yadong, Zhao Guochao, Lv Yang, Nuerxiati Abulimiti, Li Jian-Ang, Wang Dansong, Xu Xuefeng, Kuang Tiantao, Wang Xiaolin, Lou Wenhui, Liu Lingxiao, Wu Wenchuan
Department of General Surgery, Zhongshan Hospital, Institute of General Surgery and Shanghai Medical College, Fudan University, Shanghai, 200032, People's Republic of China.
Department of Interventional Radiology, Zhongshan Hospital and Shanghai Medical College, Fudan University, Shanghai, 200032, People's Republic of China.
J Cancer. 2017 Sep 20;8(16):3362-3370. doi: 10.7150/jca.20917. eCollection 2017.
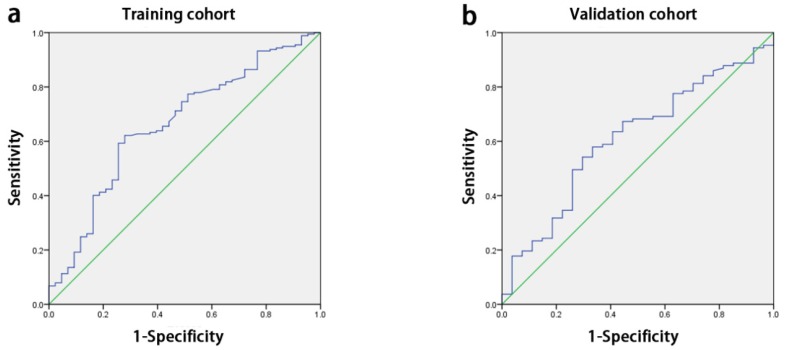
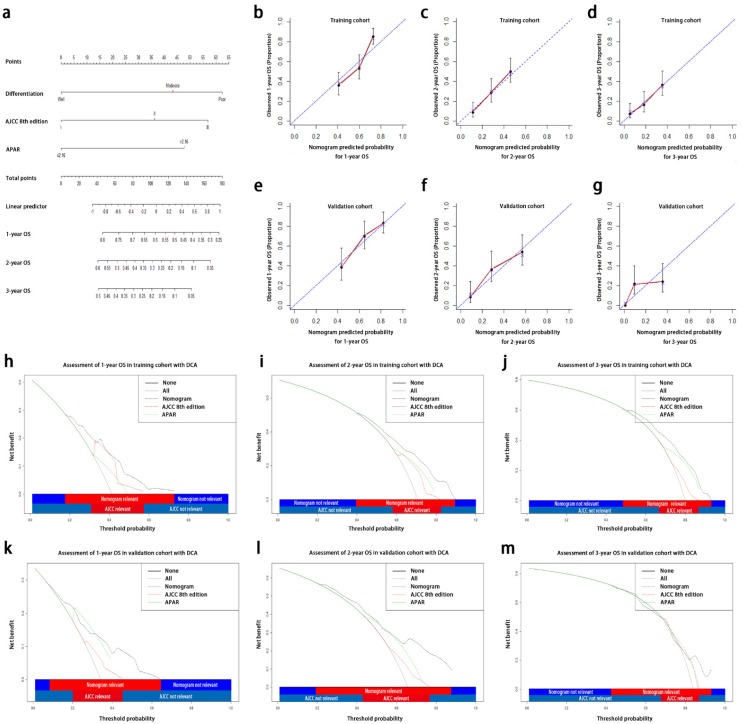
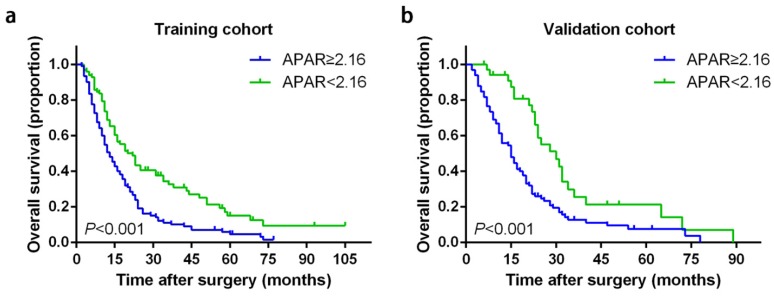
: The prognosis of pancreatic ductal adenocarcinoma (PDAC) remains poor and the models for survival prediction in PDAC patients after curative resection are still limited. Preoperative alkaline phosphatase-to-albumin ratio (APAR), an original inflammation-based score, has been established to analyze the prognostic significance in PDAC. Therefore, in this study, we aim to formulate a valuable prognostic nomogram for PDAC following curative resection. : A total of 354 patients with PDAC undergoing curative resection were retrospectively enrolled in this study. The prognostic value of APAR was analyzed in primary cohort containing 220 randomly selected PDAC patients with curative resection and prognostic nomogram incorporating APAR into the American Joint Commission on Cancer (AJCC) 8 edition was established to obtain superior discriminatory abilities. The predictive performance of APAR was further validated in another independent cohort of 134 PDAC patients. : Patients with higher serum APAR level were probable to sustain poorer overall survival (OS). Significant positive correlations were found between APAR and tumor site, and several serum biochemical indexes, such as aspartate aminotransferase (AST), alanine aminotransferase (ALT), etc. The results of multivariate analysis showed, APAR was also identified as an independent prognostic indicator for OS in both primary and validation cohorts (P=0.004, P=0.038, respectively). Compared with the AJCC 8 edition, the nomogram consisting of APAR, pathological differentiation and the TNM staging system of AJCC 8 edition showed superior predictive accuracy for OS. All these results were further verified in the validation cohort. : APAR can be considered as a novel independent prognostic biomarker for PDAC following curative resection. One more accurate and advanced predictive model will be achieved via the incorporation of APAR into nomogram.
胰腺导管腺癌(PDAC)的预后仍然很差,根治性切除术后PDAC患者的生存预测模型仍然有限。术前碱性磷酸酶与白蛋白比值(APAR)是一种基于炎症的原始评分,已被用于分析PDAC的预后意义。因此,在本研究中,我们旨在为根治性切除术后的PDAC制定一个有价值的预后列线图。
本研究回顾性纳入了354例接受根治性切除的PDAC患者。在包含220例随机选择的接受根治性切除的PDAC患者的初级队列中分析了APAR的预后价值,并建立了将APAR纳入美国癌症联合委员会(AJCC)第8版的预后列线图,以获得更好的区分能力。在另一个由134例PDAC患者组成的独立队列中进一步验证了APAR的预测性能。
血清APAR水平较高的患者总体生存期(OS)可能较差。发现APAR与肿瘤部位以及一些血清生化指标,如天冬氨酸转氨酶(AST)、丙氨酸转氨酶(ALT)等之间存在显著正相关。多因素分析结果显示,在初级队列和验证队列中,APAR均被确定为OS的独立预后指标(分别为P = 0.004,P = 0.038)。与AJCC第8版相比,由APAR、病理分化和AJCC第8版TNM分期系统组成的列线图对OS显示出更好的预测准确性。所有这些结果在验证队列中得到了进一步验证。
APAR可被视为根治性切除术后PDAC的一种新型独立预后生物标志物。通过将APAR纳入列线图将实现一个更准确、更先进的预测模型。