Raihan Ruksana
Faculty of Medicine, Aimst University, Kedah, Malaysia.
Euroasian J Hepatogastroenterol. 2016 Jan-Jun;6(1):52-55. doi: 10.5005/jp-journals-10018-1167. Epub 2016 Jul 9.
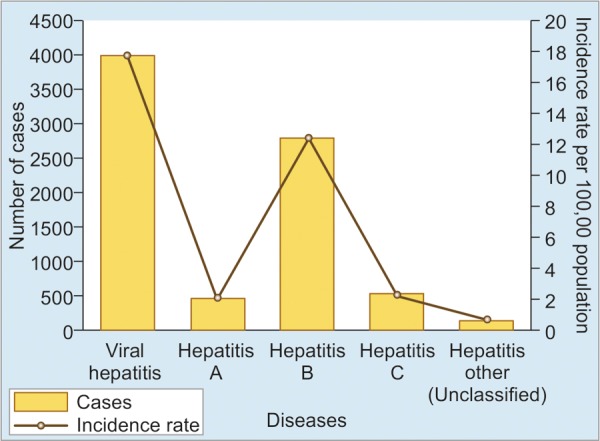
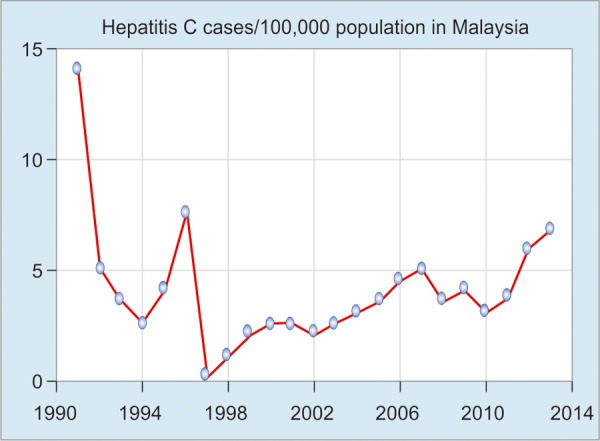
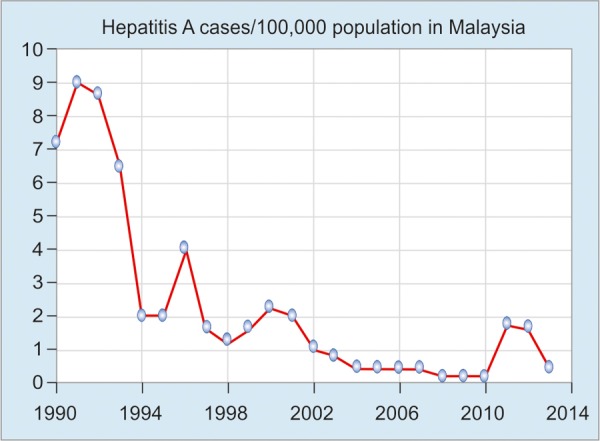
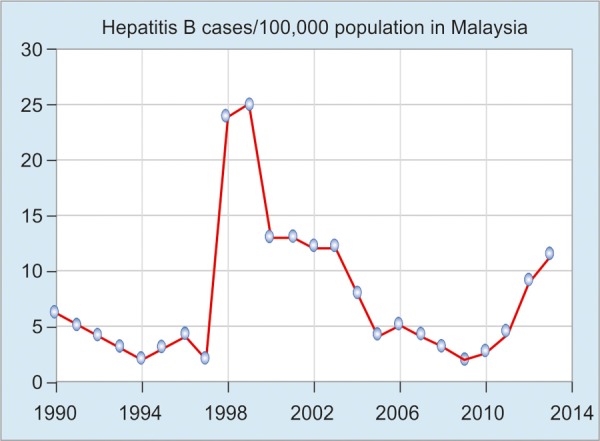
Malaysia is multiethnic, with a population of 31,127,247 comprising a mixture of Malays (50.1%), Chinese (22.6%), Indians (6.7%), Aborigines (11.8%), others (0.7%), and noncitizens (8.2%). Like other countries in the region, viral hepatitis is an important public health problem in Malaysia. The 3 most common causes for hepatitis in Malaysia are hepatitis A, B, and C. Hepatitis A has been a reportable disease in Malaysia since 1988. Due to the introduction of government control programs, the national incidence rate has dropped steadily. It is now estimated that 50% of Malaysians less than 30 years of age do not have antibodies to hepatitis A and are therefore susceptible to the disease, which can be prevented by reinforcing the hygiene status of the general population. Malaysia is a country of medium seroprevalence for the hepatitis B virus (HBV) surface antigen (HBsAg) in the general population (1.5-9.8%). The major route of transmission is from infected mother to fetus. There are an estimated 1 million people chronically infected with hepatitis B in Malaysia. Approximately 75% of all viral hepatitis cases are due to hepatitis B infection, with a male-to-female ratio of 2:1. Chronic hepatitis B (CHB) accounts for more than 80% of the hepatocellular carcinoma (HCC) cases seen in Malaysia and HCC is the 3rd most common malignant neoplasm and among the 10 leading causes of death. Most common genotypes are B and C. Incidence rates among Chinese, Malays, and Indians are 36, 26, and 15% respectively. The hepatitis B vaccination program for children was introduced in 1989, which successfully managed to reduce the seroprevalence of infection among Malaysians to 0.01% (graph 4, 2014). But the disease burden will still remain high for some time as the infected people are getting older and living longer. Hepatitis C virus (HCV) infection is a growing problem in Malaysia. An estimated 453,700 people were living with HCV infection in Malaysia in 2009 (2.5% of the population aged 15-64 years), of whom 59% acquired their infection through injection and the most common genotypes found are genotype 3 and 1. The HCV-related disease burden is already high and is forecast to rise steeply over the coming decades under current levels of antiviral treatment. Increased governmental resources to improve HCV screening and treatment rates and to reduce transmission are essential to address the high projected HCV disease burden in Malaysia.
Raihan R. Hepatitis in Malaysia: Past, Present, and Future. Euroasian J Hepato-Gastroenterol 2016;6(1):52-55.
马来西亚是一个多民族国家,人口为31,127,247,由马来人(50.1%)、华人(22.6%)、印度人(6.7%)、原住民(11.8%)、其他人(0.7%)和非公民(8.2%)组成。与该地区的其他国家一样,病毒性肝炎是马来西亚一个重要的公共卫生问题。马来西亚肝炎的3种最常见病因是甲型、乙型和丙型肝炎。自1988年以来,甲型肝炎在马来西亚一直是应报告的疾病。由于政府控制项目的实施,全国发病率稳步下降。据估计,30岁以下的马来西亚人中有50%没有甲型肝炎抗体,因此易感染该病,可通过加强普通人群的卫生状况来预防。马来西亚是普通人群中乙型肝炎病毒(HBV)表面抗原(HBsAg)血清流行率中等的国家(1.5 - 9.8%)。主要传播途径是从感染母亲传给胎儿。马来西亚估计有100万人慢性感染乙型肝炎。所有病毒性肝炎病例中约75%是由乙型肝炎感染引起的,男女比例为2:1。慢性乙型肝炎(CHB)占马来西亚肝细胞癌(HCC)病例的80%以上,HCC是第三大常见恶性肿瘤,也是十大主要死因之一。最常见的基因型是B和C。华人、马来人和印度人的发病率分别为36%、26%和15%。1989年开始实施儿童乙型肝炎疫苗接种计划,该计划成功地将马来西亚人感染的血清流行率降低到了0.01%(图4,2014年)。但由于感染者年龄增长且寿命延长,疾病负担在一段时间内仍将居高不下。丙型肝炎病毒(HCV)感染在马来西亚是一个日益严重的问题。2009年,马来西亚估计有453,700人感染HCV(占15 - 64岁人口的2.5%),其中59%通过注射感染,最常见的基因型是3型和1型。与HCV相关的疾病负担已经很高,预计在当前抗病毒治疗水平下,未来几十年还将急剧上升。增加政府资源以提高HCV筛查和治疗率并减少传播,对于应对马来西亚预计的高HCV疾病负担至关重要。
Raihan R. 马来西亚的肝炎:过去、现在和未来。《欧亚肝脏胃肠病学杂志》2016;6(1):52 - 55。