Chen Huaizhen, Busse Laurence William
Department of Medicine, Division of Pulmonary, Critical Care, Allergy and Sleep Medicine, Emory University School of Medicine, Atlanta, Georgia, USA.
Kidney Int Rep. 2017 Jun 28;2(5):785-799. doi: 10.1016/j.ekir.2017.06.020. eCollection 2017 Sep.
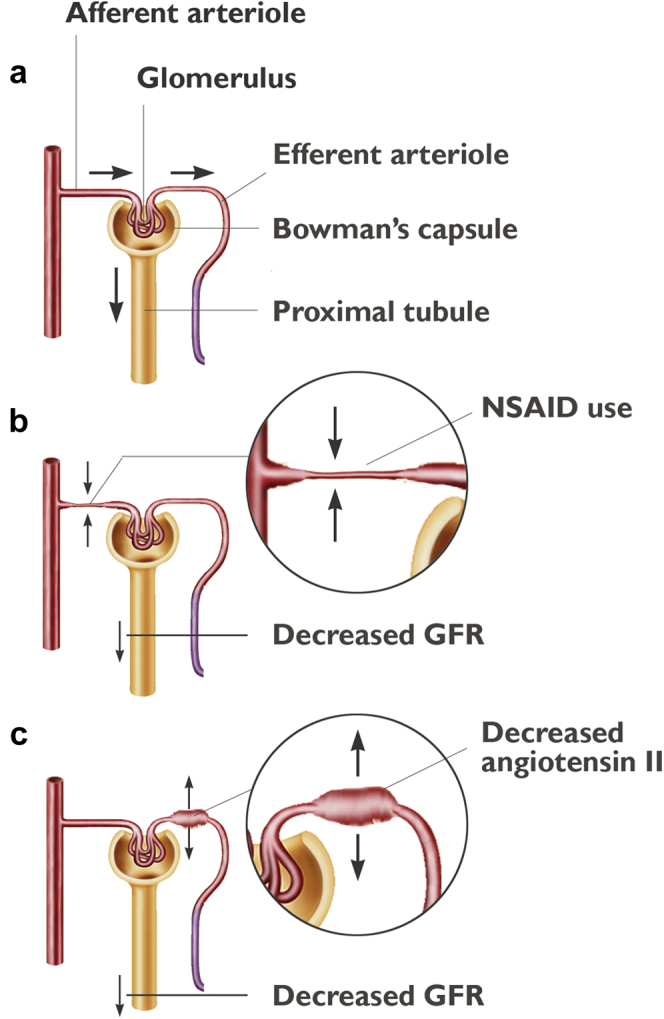
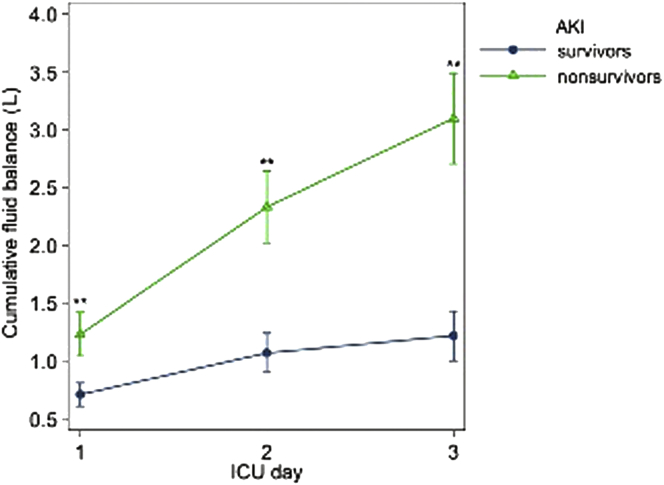
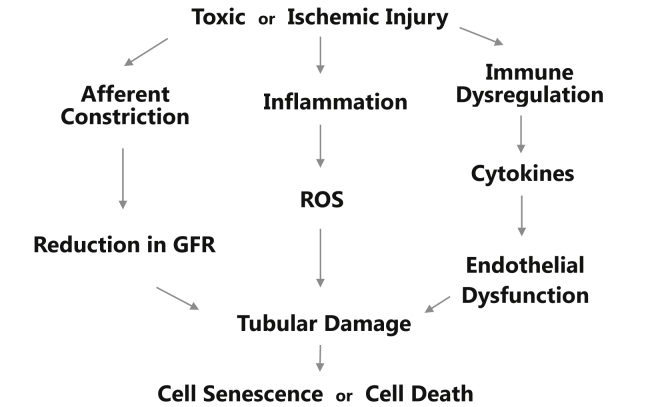
Acute kidney injury (AKI) is a common disease with a complex pathophysiology. The old paradigm of identifying renal injury based on location-prerenal, intrarenal, and postrenal-is now being supplanted with a new paradigm based on observable kidney injury patterns. The pathophysiology of AKI on a molecular and microanatomical level includes inflammation, immune dysregulation, oxidative injury, and impaired microcirculation. Treatment has traditionally been supportive, including the avoidance of nephrotoxins, judicious volume and blood pressure management, hemodynamic monitoring, and renal replacement therapy. Fluid overload and chloride-rich fluids are now implicated in the development of AKI, and resuscitation with a balanced, buffered solution at a conservative rate will mitigate risk. Novel therapies, which address specific observable kidney injury patterns include direct oxygen-free radical scavengers such as α-lipoic acid, curcumin, sodium-2-mercaptoethane sulphonate, propofol, and selenium. In addition, angiotensin II and adenosine receptor antagonists hope to ameliorate kidney injury via manipulation of renal hemodynamics and tubulo-glomerular feedback. Alkaline phosphatase, sphingosine 1 phosphate analogues, and dipeptidylpeptidase-4 inhibitors counteract kidney injury via manipulation of inflammatory pathways. Finally, genetic modifiers such as 5INP may mitigate AKI via transcriptive processes.
急性肾损伤(AKI)是一种常见疾病,其病理生理学复杂。过去基于肾前性、肾性和肾后性部位来识别肾损伤的模式,如今正被基于可观察到的肾损伤模式的新范式所取代。AKI在分子和微观解剖水平上的病理生理学包括炎症、免疫失调、氧化损伤和微循环受损。传统的治疗方法是支持性的,包括避免使用肾毒素、合理进行容量和血压管理、血流动力学监测以及肾脏替代治疗。液体超负荷和富含氯化物的液体现在被认为与AKI的发生有关,以保守速率使用平衡的缓冲溶液进行复苏将降低风险。针对特定可观察到的肾损伤模式的新型疗法包括直接的氧自由基清除剂,如α-硫辛酸、姜黄素、2-巯基乙烷磺酸钠、丙泊酚和硒。此外,血管紧张素II和腺苷受体拮抗剂希望通过调节肾血流动力学和肾小管-肾小球反馈来改善肾损伤。碱性磷酸酶、1-磷酸鞘氨醇类似物和二肽基肽酶-4抑制剂通过调节炎症途径来对抗肾损伤。最后,诸如5INP等基因修饰剂可能通过转录过程减轻AKI。