Life Course Epidemiology and Biostatistics Section, UCL GOS Institute of Child Health, London, UK.
Ulverscroft Vision Research Group, London, UK.
Br J Ophthalmol. 2018 Oct;102(10):1407-1412. doi: 10.1136/bjophthalmol-2017-311557. Epub 2018 Feb 3.
Refractive error is an increasing global public health concern that requires robust and reliable research to identify modifiable risk factors and provide accurate estimates of population burden. We investigated the impact of reclassification of individuals when using different threshold values of spherical equivalent (SE) to define myopia, on estimates of frequency, distribution and associations with risk factors, to inform current international initiatives to standardise definitions.
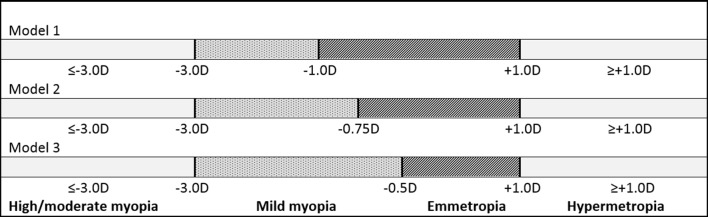
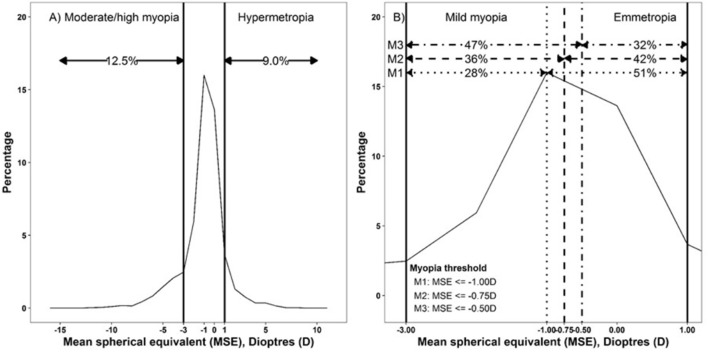
A random sample of 1985 individuals from the 1958 British birth cohort, at age 44, had autorefraction and self-reported on educational attainment and social class.Refraction status assigned in three different models using SE: (A) moderate to high myopia -3 diopters (D) or more extreme (≤-3.00D), (B) hypermetropia +1.00D or more extreme (≥+1.00D) and (C) mild myopia using three different thresholds: -1.00D, -0.75D or -0.50D, hence reciprocal changes in definition of emmetropia.
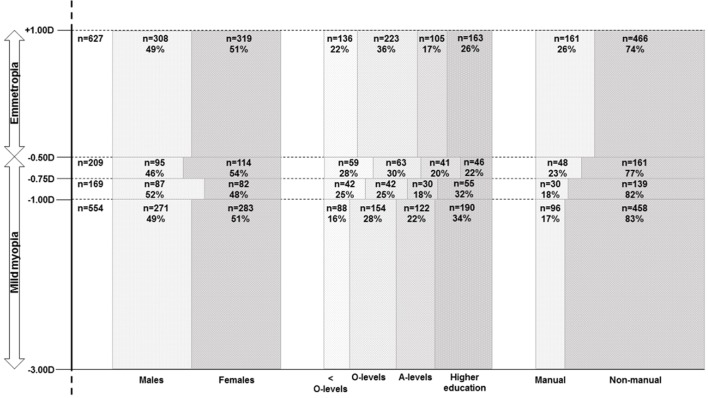
Frequency estimates and associations with risk factors altered significantly as the threshold value for myopia moved towards SE 0.0D: prevalence of mild myopia increased from 28% to 47%, the association with highest educational attainment attenuated and with higher social class strengthened, with changes in risk ratios of approximately 20%.
Even small changes in the threshold definition of myopia (±0.25D) can significantly affect the conclusions of epidemiological studies, creating both false-positive and false-negative associations for specific risk factors. An international classification for refractive error, empirically evidenced and cognisant of the question(s) being addressed and the population(s) being studied, is needed to serve better translational research, practice and policy.
屈光不正(refractive error)是一个日益严重的全球公共卫生问题,需要强有力且可靠的研究来确定可改变的危险因素,并对人群负担进行准确估计。我们研究了使用不同等效球镜(spherical equivalent,SE)阈值来定义近视时,个体分类的变化对频率、分布和与危险因素关联的估计值的影响,以便为当前国际标准化定义的举措提供信息。
1958 年英国出生队列的 1985 名随机个体在 44 岁时进行了自动折射,并报告了教育程度和社会阶层。使用 SE 将折射状态分配到三种不同的模型中:(A)中高度近视-3 屈光度(D)或更极端(≤-3.00D);(B)远视+1.00D 或更极端(≥+1.00D);(C)使用三种不同的阈值定义轻度近视:-1.00D、-0.75D 或-0.50D,因此正视的定义发生了相反的变化。
随着近视的阈值向 SE 0.0D 移动,频率估计值和与危险因素的关联发生了显著变化:轻度近视的患病率从 28%增加到 47%,与最高教育程度的关联减弱,与较高社会阶层的关联增强,风险比的变化约为 20%。
即使近视阈值的微小变化(±0.25D)也会显著影响流行病学研究的结论,为特定危险因素创造了假阳性和假阴性关联。需要一种基于经验的、考虑到所提出的问题和研究人群的屈光不正国际分类,以更好地服务于转化研究、实践和政策。