Cohen Bernard, Yakushin Sergei B, Cho Catherine
Department of Neurology, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Department of Neurology, NYU School of Medicine, New York, NY, United States.
Front Neurol. 2018 Feb 5;9:28. doi: 10.3389/fneur.2018.00028. eCollection 2018.
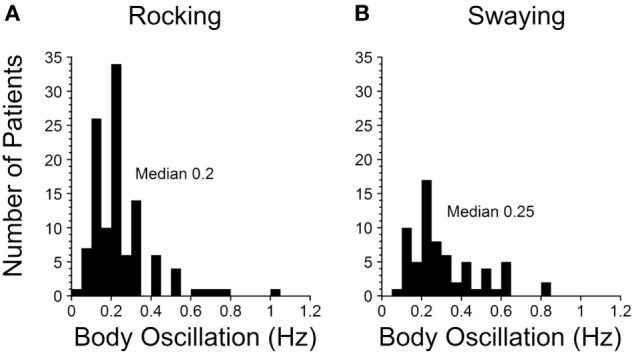
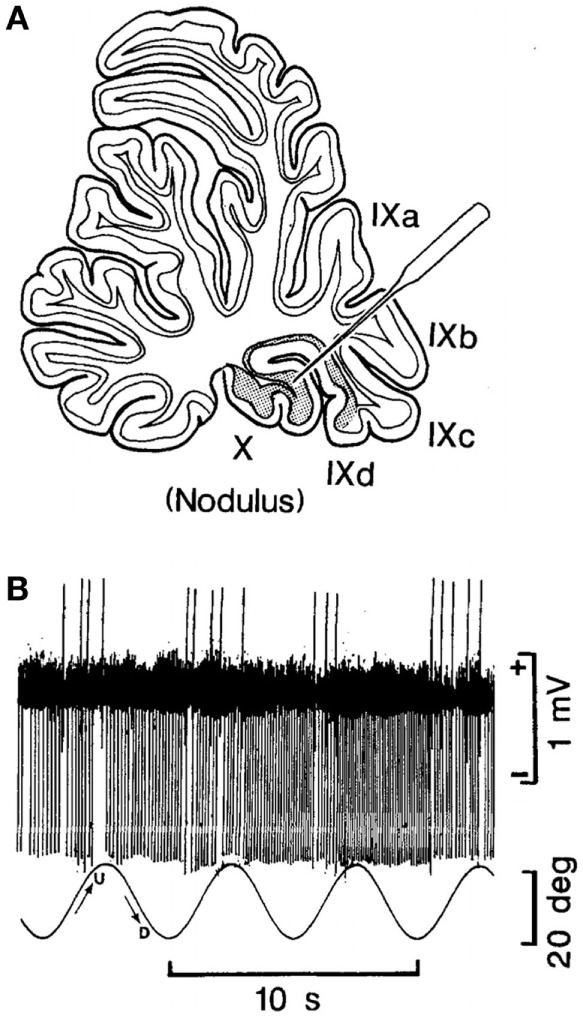
The Mal de Debarquement syndrome (MdDS) generally follows sea voyages, but it can occur after turbulent flights or spontaneously. The primary features are objective or perceived continuous rocking, swaying, and/or bobbing at 0.2 Hz after sea voyages or 0.3 Hz after flights. The oscillations can continue for months or years and are immensely disturbing. Associated symptoms appear to be secondary to the incessant sensation of movement. We previously suggested that the illness can be attributed to maladaptation of the velocity storage integrator in the vestibular system, but the actual neural mechanisms driving the MdDS are unknown. Here, based on experiments in subhuman primates, we propose a series of postulates through which the MdDS is generated: (1) The MdDS is produced in the velocity storage integrator by activation of vestibular-only (VO) neurons on either side of the brainstem that are oscillating back and forth at 0.2 or 0.3 Hz. (2) The groups of VO neurons are driven by signals that originate in Purkinje cells in the cerebellar nodulus. (3) Prolonged exposure to roll, either on the sea or in the air, conditions the roll-related neurons in the nodulus. (4) The prolonged exposure causes a shift of the pitch orientation vector from its original position aligned with gravity to a position tilted in roll. (5) Successful treatment involves exposure to a full-field optokinetic stimulus rotating around the spatial vertical countering the direction of the vestibular imbalance. This is done while rolling the head at the frequency of the perceived rocking, swaying, or bobbing. We also note experiments that could be used to verify these postulates, as well as considering potential flaws in the logic. Important unanswered questions: (1) Why does the MdDS predominantly affect women? (2) What aspect of roll causes the prolongation of the tilted orientation vector, and why is it so prolonged in some individuals? (3) What produces the increase in symptoms of some patients when returning home after treatment, and how can this be avoided? We also posit that the same mechanisms underlie the less troublesome and shorter duration Mal de Debarquement.
晕船后综合征(MdDS)通常发生在海上航行之后,但也可能在颠簸的飞行后或自发出现。其主要特征是在海上航行后出现频率为0.2赫兹的客观或主观感受到的持续摇晃、摆动和/或颠簸,或在飞行后出现频率为0.3赫兹的上述情况。这些振荡可能持续数月或数年,令人极为困扰。相关症状似乎是由持续的运动感觉继发而来。我们之前曾提出,该疾病可归因于前庭系统中速度存储积分器的适应不良,但驱动MdDS的实际神经机制尚不清楚。在此,基于对非人灵长类动物的实验,我们提出了一系列关于MdDS产生的假设:(1)MdDS是由脑干两侧仅对前庭刺激有反应(VO)的神经元激活速度存储积分器产生的,这些神经元以0.2或0.3赫兹的频率来回振荡。(2)VO神经元群由源自小脑蚓部浦肯野细胞的信号驱动。(3)长时间暴露于海上或空中的横摇会使蚓部与横摇相关的神经元产生条件反射。(4)长时间暴露会导致俯仰方向向量从与重力对齐的原始位置偏移到在横摇中倾斜的位置。(5)成功的治疗包括暴露于围绕空间垂直轴旋转的全视野视动刺激,其旋转方向与前庭不平衡方向相反。在以感觉到的摇晃、摆动或颠簸频率转动头部的同时进行此操作。我们还提到了可用于验证这些假设的实验,并考虑了逻辑上的潜在缺陷。重要的未解决问题:(1)为什么MdDS主要影响女性?(2)横摇的哪个方面导致倾斜方向向量延长,为什么在某些个体中延长如此明显?(3)一些患者在治疗后回家时症状为何会加重,如何避免这种情况?我们还假定,同样的机制是导致症状较轻、持续时间较短的晕船后综合征的基础。