Cranmer John N, Dettinger Julia, Calkins Kimberly, Kibore Minnie, Gachuno Onesmus, Walker Dilys
Emory University, Atlanta, Georgia, United States of America.
University of Washington, Department of Global Health, Seattle, Washington, United States of America.
PLoS One. 2018 Feb 23;13(2):e0184252. doi: 10.1371/journal.pone.0184252. eCollection 2018.
Globally, the rate of reduction in delivery-associated maternal and perinatal mortality has been slow compared to improvements in post-delivery mortality in children under five. Improving clinical readiness for basic obstetric emergencies is crucial for reducing facility-based maternal deaths. Emergency readiness is commonly assessed using tracers derived from the maternal signal functions model.
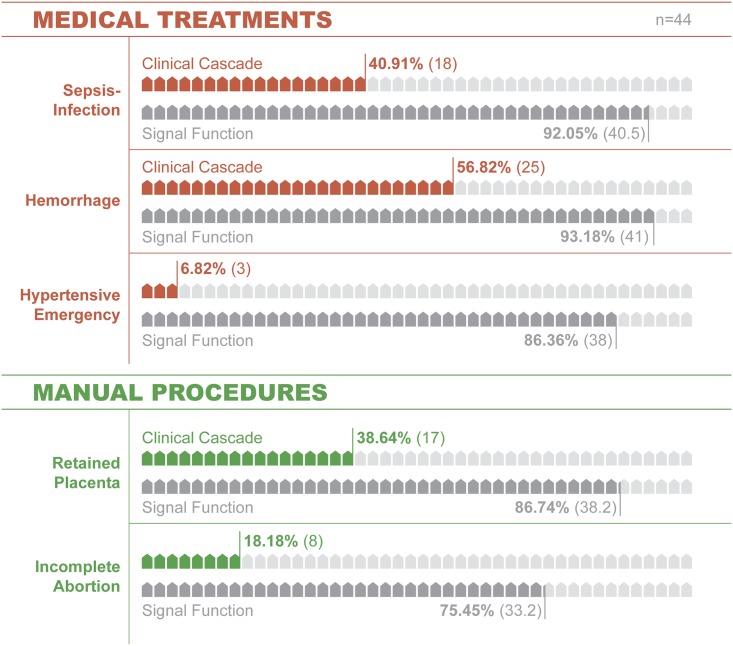
OBJECTIVE-METHOD: We compare emergency readiness using the signal functions model and a novel clinical cascade. The cascades model readiness as the proportion of facilities with resources to identify the emergency (stage 1), treat it (stage 2) and monitor-modify therapy (stage 3). Data were collected from 44 Kenyan clinics as part of an implementation trial.
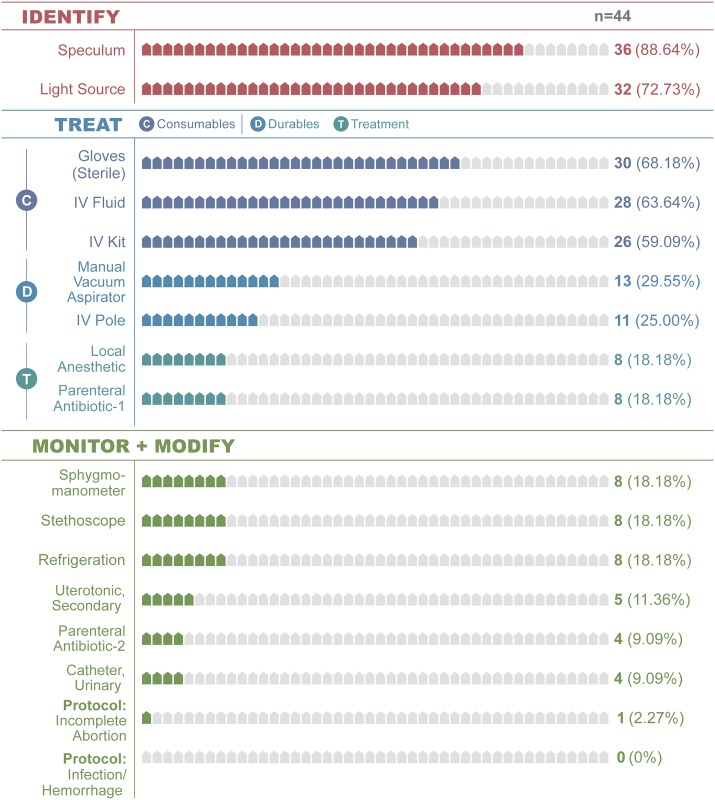
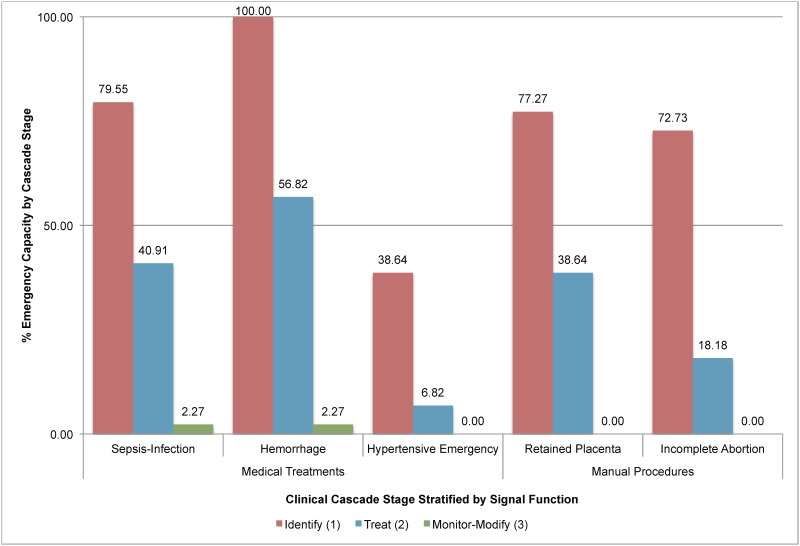
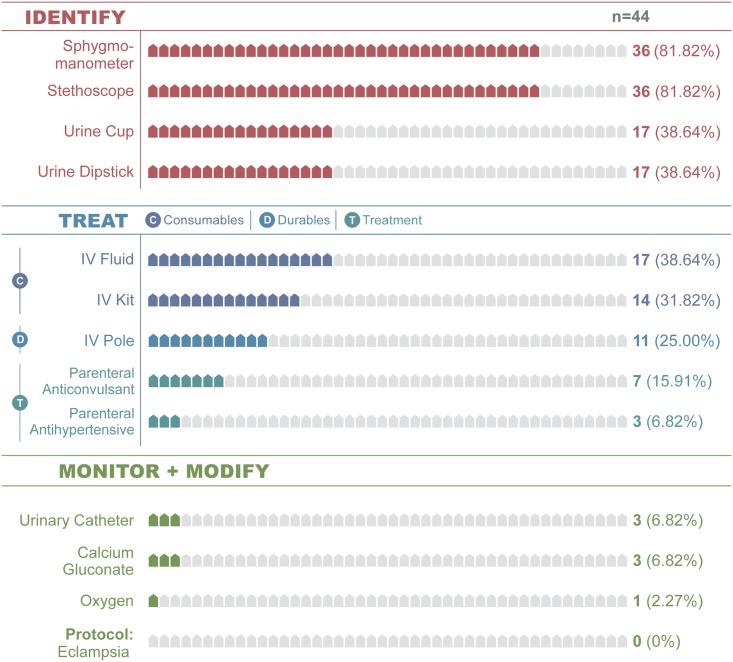
Although most facilities (77.0%) stock maternal signal function tracer drugs, far fewer have resources to practically identify and treat emergencies. In hypertensive emergencies for example, 38.6% of facilities have resources to identify the emergency (Stage 1 readiness, including sphygmomanometer, stethoscope, urine collection device, protein test). 6.8% have the resources to treat the emergency (Stage 2, consumables (IV Kit, fluids), durable goods (IV pole) and drugs (magnesium sulfate and hydralazine). No facilities could monitor or modify therapy (Stage 3). Across five maternal emergencies, the signal functions overestimate readiness by 54.5%. A consistent, step-wise pattern of readiness loss across signal functions and care stage emerged and was profoundly consistent at 33.0%.
Comparing estimates from the maternal signal functions and cascades illustrates four themes. First, signal functions overestimate practical readiness by 55%. Second, the cascade's intuitive indicators can support cross-sector health system or program planners to more precisely measure and improve emergency care. Third, adding few variables to existing readiness inventories permits step-wise modeling of readiness loss and can inform more precise interventions. Fourth, the novel aggregate readiness loss indicator provides an innovative and intuitive approach for modeling health system emergency readiness. Additional testing in diverse contexts is warranted.
在全球范围内,与五岁以下儿童产后死亡率的改善相比,分娩相关的孕产妇和围产期死亡率的下降速度一直较慢。提高对基本产科紧急情况的临床准备程度对于降低医疗机构内的孕产妇死亡至关重要。应急准备通常使用源自孕产妇信号功能模型的追踪指标进行评估。
目的-方法:我们使用信号功能模型和一种新型临床级联来比较应急准备情况。级联将准备情况建模为具备识别紧急情况(第1阶段)、治疗紧急情况(第2阶段)以及监测-调整治疗(第3阶段)资源的设施所占比例。作为一项实施试验的一部分,我们从44家肯尼亚诊所收集了数据。
尽管大多数设施(77.0%)储备了孕产妇信号功能追踪药物,但实际具备识别和治疗紧急情况资源的设施要少得多。例如,在高血压紧急情况中,38.6%的设施具备识别紧急情况的资源(第1阶段准备情况,包括血压计、听诊器、尿液收集装置、蛋白质检测)。6.8%的设施具备治疗紧急情况的资源(第2阶段,消耗品(静脉输液套件、液体)、耐用物品(静脉输液杆)和药物(硫酸镁和肼屈嗪))。没有设施能够监测或调整治疗(第3阶段)。在五种孕产妇紧急情况中,信号功能将准备情况高估了54.5%。在信号功能和护理阶段出现了一种一致的、逐步的准备情况丧失模式,且在33.0%时高度一致。
比较孕产妇信号功能和级联的评估结果说明了四个主题。第一,信号功能将实际准备情况高估了55%。第二,级联直观的指标可以支持跨部门卫生系统或项目规划者更精确地衡量和改善紧急护理。第三,在现有的准备情况清单中添加少量变量可以对应急准备情况丧失进行逐步建模,并可为更精确的干预措施提供参考。第四,新型的总体应急准备情况丧失指标为卫生系统应急准备情况建模提供了一种创新且直观的方法。有必要在不同背景下进行更多测试。