van Dijk S T, Bos K, de Boer M G J, Draaisma W A, van Enst W A, Felt R J F, Klarenbeek B R, Otte J A, Puylaert J B C M, van Geloven A A W, Boermeester M A
Department of Surgery, Academic Medical Center, Amsterdam, the Netherlands.
Department of Infectious Diseases, Leiden University Medical Center, Leiden, the Netherlands.
Int J Colorectal Dis. 2018 May;33(5):505-512. doi: 10.1007/s00384-018-3015-9. Epub 2018 Mar 12.
The shift from routine antibiotics towards omitting antibiotics for uncomplicated acute diverticulitis opens up the possibility for outpatient instead of inpatient treatment, potentially reducing the burden of one of the most common gastrointestinal diseases in the Western world.
Assessing the safety and cost savings of outpatient treatment in acute colonic diverticulitis.
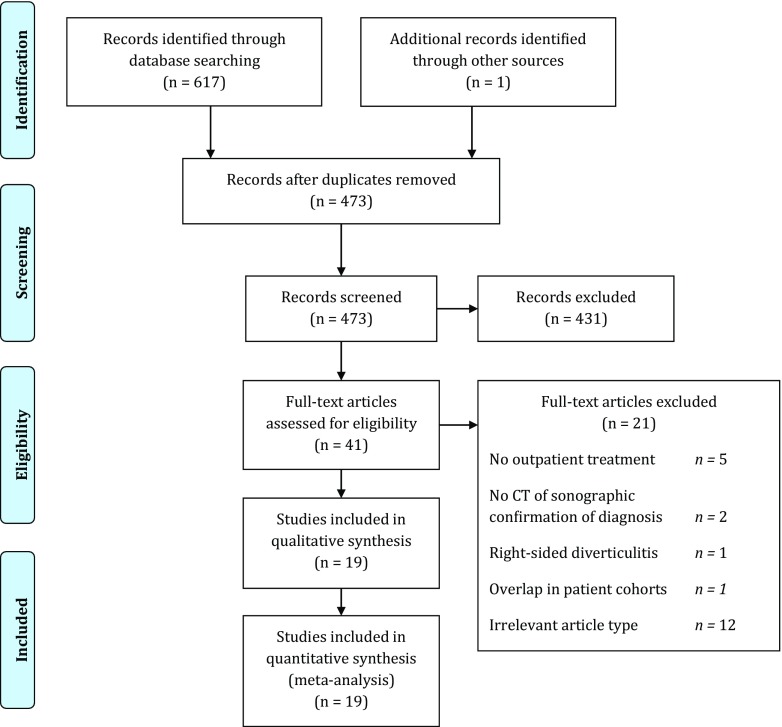
PubMed and EMBASE were searched for studies on outpatient treatment of colonic diverticulitis, confirmed with computed tomography or ultrasound. Outcomes were readmission rate, need for emergency surgery or percutaneous abscess drainage, and healthcare costs.
A total of 19 studies with 2303 outpatient treated patients were included. These studies predominantly excluded patients with comorbidity or immunosuppression, inability to tolerate oral intake, or lack of an adequate social network. The pooled incidence rate of readmission for outpatient treatment was 7% (95%CI 6-9%, I 48%). Only 0.2% (2/1288) of patients underwent emergency surgery, and 0.2% (2/1082) of patients underwent percutaneous abscess drainage. Only two studies compared readmission rates outpatients that had similar characteristics as a control group of inpatients; 4.5% (3/66) and 6.3% (2/32) readmissions in outpatient groups versus 6.1% (4/66) and 0.0% (0/44) readmissions in inpatient groups (p = 0.619 and p = 0.174, respectively). Average healthcare cost savings for outpatient compared with inpatient treatment ranged between 42 and 82%.
Outpatient treatment of uncomplicated diverticulitis resulted in low readmission rates and very low rates of complications. Furthermore, healthcare cost savings were substantial. Therefore, outpatient treatment of uncomplicated diverticulitis seems to be a safe option for most patients.
从常规使用抗生素转向对单纯性急性憩室炎不使用抗生素,为门诊治疗而非住院治疗开辟了可能性,这有可能减轻西方世界最常见的胃肠道疾病之一的负担。
评估急性结肠憩室炎门诊治疗的安全性和成本节约情况。
检索PubMed和EMBASE上关于经计算机断层扫描或超声确诊的结肠憩室炎门诊治疗的研究。结果指标为再入院率、急诊手术或经皮脓肿引流的需求以及医疗费用。
共纳入19项研究,涉及2303例接受门诊治疗的患者。这些研究主要排除了合并症或免疫抑制患者、无法耐受口服摄入者或缺乏足够社会支持网络的患者。门诊治疗的再入院合并发生率为7%(95%置信区间6 - 9%,I² = 48%)。仅0.2%(2/1288)的患者接受了急诊手术,0.2%(2/1082)的患者接受了经皮脓肿引流。只有两项研究比较了具有与住院患者对照组相似特征的门诊患者的再入院率;门诊组的再入院率为4.5%(3/66)和6.3%(2/32),而住院组为6.1%(4/66)和0.0%(0/44)(p分别为0.619和0.174)。与住院治疗相比,门诊治疗平均节省的医疗费用在42%至82%之间。
单纯性憩室炎的门诊治疗导致再入院率低且并发症发生率极低。此外,医疗费用大幅节省。因此,对于大多数患者而言,单纯性憩室炎的门诊治疗似乎是一种安全的选择。